Anda mungkin juga menyukai
- 0001 CatDokumen108 halaman0001 CatJorge CabreraBelum ada peringkat
- 432 HZ - Unearthing The Truth Behind Nature's FrequencyDokumen6 halaman432 HZ - Unearthing The Truth Behind Nature's FrequencyShiv KeskarBelum ada peringkat
- Asme NM.2-2018Dokumen126 halamanAsme NM.2-2018aneeshjokay75% (4)
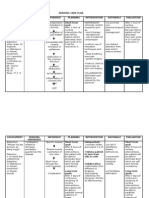
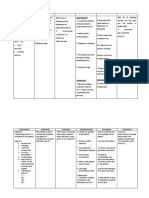
- Nursing Care Plan Format Name: - Medical Diagnosis: Myasthenia Gravis DateDokumen2 halamanNursing Care Plan Format Name: - Medical Diagnosis: Myasthenia Gravis DateSheryl Ann Barit Pedines100% (1)
- Lines WorksheetDokumen3 halamanLines WorksheetJuzef StaljinBelum ada peringkat
- Nursing Cues for Pain ManagementDokumen8 halamanNursing Cues for Pain ManagementAi RouBelum ada peringkat
- The Motive Journal (3rd Edition)Dokumen42 halamanThe Motive Journal (3rd Edition)Shubham Sharma0% (1)
- S6MT 1Q w1 3 MELC1 SLM MIXTURES FinalCopy09082020Dokumen26 halamanS6MT 1Q w1 3 MELC1 SLM MIXTURES FinalCopy09082020Rona Dindang100% (1)
- Self Care DeficitDokumen4 halamanSelf Care DeficitEllaine RamirezBelum ada peringkat
- Age Discrimination PDFDokumen20 halamanAge Discrimination PDFMd. Rezoan ShoranBelum ada peringkat
- Keys To Biblical CounselingDokumen7 halamanKeys To Biblical CounselingDavid Salazar100% (6)
- NCP Icu-CcuDokumen6 halamanNCP Icu-CcuJohn CenasBelum ada peringkat
- NCP Gouty ArthritisDokumen21 halamanNCP Gouty ArthritisArianne Kamille Andes67% (3)
- NCP CvaDokumen3 halamanNCP CvaJey PangilinanBelum ada peringkat
- NCP Inffective Tissue PerfusionDokumen3 halamanNCP Inffective Tissue PerfusionPaul Cubacub0% (1)
- Tachycardia NCPDokumen2 halamanTachycardia NCPRemita Hutagalung50% (4)
- NCP - CvaDokumen3 halamanNCP - CvaBrenda Lee0% (1)
- NCP StrokeDokumen2 halamanNCP StrokeMichael John F. NatividadBelum ada peringkat
- The Philippine Health Care Delivery SystemDokumen7 halamanThe Philippine Health Care Delivery SystemJoselene Arenas DeDios95% (41)
- NCP Ischemic StrokeDokumen3 halamanNCP Ischemic StrokeLP Benoza100% (3)
- NCP - ConstipationDokumen3 halamanNCP - ConstipationDaniel Dave KapunanBelum ada peringkat
- NCP For StrokeDokumen4 halamanNCP For StrokeJASON OGALESCOBelum ada peringkat
- A1 Cp-Self Care DeficitDokumen7 halamanA1 Cp-Self Care DeficitCherryjuliejane Rosales CaperidaBelum ada peringkat
- NCP Risk For InjuryDokumen2 halamanNCP Risk For InjuryAbigail Joy Tabones75% (4)
- Name of Drug Dosage/Route Mechanism of Action/ Classification Indication/Contraindication Side/Adverse Effects Nursing ConsiderationsDokumen3 halamanName of Drug Dosage/Route Mechanism of Action/ Classification Indication/Contraindication Side/Adverse Effects Nursing ConsiderationsMonica Gagarin CortezBelum ada peringkat
- NCP: Patient With A Pressure UlcerDokumen2 halamanNCP: Patient With A Pressure UlcerICa MarlinaBelum ada peringkat
- Target ListDokumen9 halamanTarget ListChaitali DegavkarBelum ada peringkat
- SchistosomiasisDokumen92 halamanSchistosomiasisIvan Juan75% (4)
- Ineffective Tissue PerfusionDokumen2 halamanIneffective Tissue PerfusionClaidelyn De Leyola100% (1)
- NCP Activity IntoleranceDokumen5 halamanNCP Activity IntoleranceRea HashimBelum ada peringkat
- NCP IschemicDokumen19 halamanNCP IschemicChristina Espiña EjercitoBelum ada peringkat
- Hemodialysis NCPDokumen2 halamanHemodialysis NCPAfia Tawiah100% (1)
- CVA Patient AssessmentDokumen10 halamanCVA Patient AssessmentSarah BenjaminBelum ada peringkat
- NCP - Ineffective Airway ClearanceDokumen2 halamanNCP - Ineffective Airway Clearancelarapatricia1215Belum ada peringkat
- Gouty Arthritis-NcpDokumen2 halamanGouty Arthritis-NcpJohn D100% (2)
- NCP Ineffective Tissue Perfusion and Self Care DeficitDokumen5 halamanNCP Ineffective Tissue Perfusion and Self Care DeficitFrances Anne Pasiliao100% (3)
- Ineffective Renal Tissue PerfusionDokumen2 halamanIneffective Renal Tissue PerfusionHendra Tanjung100% (4)
- NCP NeuroDokumen20 halamanNCP NeuroNica Gaborne Navarro100% (3)
- NCP - Tissue Perfusion (Cerebral)Dokumen2 halamanNCP - Tissue Perfusion (Cerebral)moodlayers50% (6)
- Stroke NCPDokumen5 halamanStroke NCPChantal Caragan100% (1)
- Assessing and Managing Risk of InjuryDokumen2 halamanAssessing and Managing Risk of InjuryStar Alvarez100% (2)
- Risk For Impaired Skin Integrity and Readiness For Enhanced PowerDokumen3 halamanRisk For Impaired Skin Integrity and Readiness For Enhanced PowerdanaBelum ada peringkat
- Nursing Care Plan For CholedocholithiasisDokumen2 halamanNursing Care Plan For Choledocholithiasis_cezca_100% (3)
- Nursing Care PlanDokumen3 halamanNursing Care PlanJayalakshmi David50% (2)
- NCP For Pain - Rheumatoid ArthritisDokumen5 halamanNCP For Pain - Rheumatoid Arthritisveorjan100% (1)
- NCP Activity IntoleranceDokumen2 halamanNCP Activity Intolerancea22hous0% (1)
- NCP Tissue PerfusionDokumen4 halamanNCP Tissue PerfusionLisa Tandog100% (1)
- Activity Intolerance Related To Decrease Blood FlowDokumen3 halamanActivity Intolerance Related To Decrease Blood FlowDarkCeades100% (3)
- Ineffective Tissue PerfusionDokumen2 halamanIneffective Tissue PerfusionDiane ReyBelum ada peringkat
- Nursing Care PlanDokumen22 halamanNursing Care PlanjamBelum ada peringkat
- NCP For InfectionDokumen1 halamanNCP For InfectionNathaniel EllanoBelum ada peringkat
- NCP Acute PainDokumen5 halamanNCP Acute PainMicah Jonah Elicaño0% (1)
- Nursing Care Plan Risk For Skin BreakdownDokumen3 halamanNursing Care Plan Risk For Skin BreakdownShelli Miller Pryor82% (11)
- NCP BkaDokumen4 halamanNCP BkaKeeshia CesnerosBelum ada peringkat
- Assessment Diagnosis Planning ImplementationDokumen4 halamanAssessment Diagnosis Planning ImplementationMG PolvorosaBelum ada peringkat
- Skin Integrity Nursing Care for ElderlyDokumen2 halamanSkin Integrity Nursing Care for ElderlyRazz Domenique Reyes Escaros100% (5)
- NCPDokumen2 halamanNCPLyka Mae Imbat - PacnisBelum ada peringkat
- Ineffective Breathing PatternDokumen185 halamanIneffective Breathing PatternSusi LambiyantiBelum ada peringkat
- NCPDokumen3 halamanNCPJezza RequilmeBelum ada peringkat
- Nursing Care Plan For Impaired Environmental Interpretaion NCPDokumen4 halamanNursing Care Plan For Impaired Environmental Interpretaion NCPderic100% (2)
- Comprehensive Assessment Is Not A Neutral ProcessDokumen2 halamanComprehensive Assessment Is Not A Neutral ProcessGrape JuiceBelum ada peringkat
- NURSING CARE PLAN Problem Body Weakness Nursing Diagnosis Impaired PhysicalDokumen1 halamanNURSING CARE PLAN Problem Body Weakness Nursing Diagnosis Impaired Physicalmitchie riveraBelum ada peringkat
- NCP PROPER Pain and Decreased Cardiac OutputDokumen3 halamanNCP PROPER Pain and Decreased Cardiac OutputErienne Lae Manangan - CadalsoBelum ada peringkat
- Pneumonia Care PlanDokumen1 halamanPneumonia Care Plantcumurphish67% (3)
- Identified Nursing Diagnoses and PrioritizationDokumen4 halamanIdentified Nursing Diagnoses and Prioritizationrheinz-marlon-m-carlos-7771Belum ada peringkat
- NCP StrokeDokumen2 halamanNCP StrokeEtienne NinxBelum ada peringkat
- VIGOCIDDokumen2 halamanVIGOCIDKaren DamoBelum ada peringkat
- 217 RF Peripheral Neurovascular DysfunctionDokumen8 halaman217 RF Peripheral Neurovascular Dysfunctionapi-271775750Belum ada peringkat
- Post Operation Care After PullDokumen8 halamanPost Operation Care After PulldhagallarteBelum ada peringkat
- Nursing Care Plan - NeuroDokumen3 halamanNursing Care Plan - NeuroJohara G'naidBelum ada peringkat
- Nursing Care Plan for Skin Integrity Post-SurgeryDokumen3 halamanNursing Care Plan for Skin Integrity Post-SurgeryChristy BerryBelum ada peringkat
- Iv. Anatomy and PhysiologyDokumen5 halamanIv. Anatomy and PhysiologyMonica Gagarin CortezBelum ada peringkat
- Drug StudyDokumen2 halamanDrug StudyMonica Gagarin CortezBelum ada peringkat
- Verbal ImpairedDokumen2 halamanVerbal ImpairedWinnie EmperadorBelum ada peringkat
- Drug StudyDokumen2 halamanDrug StudyMonica Gagarin CortezBelum ada peringkat
- NCPDokumen5 halamanNCPMonica Gagarin CortezBelum ada peringkat
- App 17 Venmyn Rand Summary PDFDokumen43 halamanApp 17 Venmyn Rand Summary PDF2fercepolBelum ada peringkat
- Easy and Successful Plumbing Methods You Can Now Applyhslhj PDFDokumen2 halamanEasy and Successful Plumbing Methods You Can Now Applyhslhj PDFbeartea84Belum ada peringkat
- Class9. CVD and PVDDokumen30 halamanClass9. CVD and PVDiraBelum ada peringkat
- VERALLIA WHITE-BOOK EN March2022 PDFDokumen48 halamanVERALLIA WHITE-BOOK EN March2022 PDFEugenio94Belum ada peringkat
- Airborne Life Support Systems In-House Infant Transport Sys 185A Infant Incubator - Manufacturer SpecificationsDokumen2 halamanAirborne Life Support Systems In-House Infant Transport Sys 185A Infant Incubator - Manufacturer SpecificationsAsistir Biomedica SASBelum ada peringkat
- H1 Revision Notes DNA and GenomicsDokumen6 halamanH1 Revision Notes DNA and GenomicsJiaLi XieBelum ada peringkat
- Sugar Reseach in AustraliaDokumen16 halamanSugar Reseach in AustraliaJhonattanIsaacBelum ada peringkat
- Accuracy of Real-Time Shear Wave Elastography in SDokumen10 halamanAccuracy of Real-Time Shear Wave Elastography in SApotik ApotekBelum ada peringkat
- Temporomandibular Joint SyndromeDokumen11 halamanTemporomandibular Joint SyndromeRahma RahmaBelum ada peringkat
- 21 - Effective Pages: Beechcraft CorporationDokumen166 halaman21 - Effective Pages: Beechcraft CorporationCristian PugaBelum ada peringkat
- Undas Deployment PadsDokumen15 halamanUndas Deployment PadsVic NairaBelum ada peringkat
- Role of Homeostasis in Human Physiology A ReviewDokumen5 halamanRole of Homeostasis in Human Physiology A ReviewNathaly ZiékteBelum ada peringkat
- Arecaceae or Palmaceae (Palm Family) : Reported By: Kerlyn Kaye I. AsuncionDokumen23 halamanArecaceae or Palmaceae (Palm Family) : Reported By: Kerlyn Kaye I. AsuncionNamae BacalBelum ada peringkat
- Chin Cup Therapy An Effective Tool For The Correction of Class III Malocclusion in Mixed and Late Deciduous DentitionsDokumen6 halamanChin Cup Therapy An Effective Tool For The Correction of Class III Malocclusion in Mixed and Late Deciduous Dentitionschic organizerBelum ada peringkat
- Environmental Product Declaration: PU EuropeDokumen6 halamanEnvironmental Product Declaration: PU EuropeIngeniero Mac DonnellBelum ada peringkat
- Cement Evaluation CAST-CBL HalliburtonDokumen36 halamanCement Evaluation CAST-CBL HalliburtonrezaBelum ada peringkat
- MPQ2908 - 48V Buck Converter Automotive Reference DesignDokumen4 halamanMPQ2908 - 48V Buck Converter Automotive Reference DesignShubham KaklijBelum ada peringkat
- The Truth About EtawahDokumen4 halamanThe Truth About EtawahPoojaDasgupta100% (1)
- Heat Transfer Augmentation in Decaying Turbulent Swirl FlowDokumen1 halamanHeat Transfer Augmentation in Decaying Turbulent Swirl FlowOnkar ChavanBelum ada peringkat
- Generate Profits from Bottled Water Using Atmospheric Water GeneratorsDokumen20 halamanGenerate Profits from Bottled Water Using Atmospheric Water GeneratorsJose AndradeBelum ada peringkat
- Schneider - Cptg010 en (Print)Dokumen16 halamanSchneider - Cptg010 en (Print)el_koptan00857693Belum ada peringkat