Anda mungkin juga menyukai
- Ebstein Anomaly, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDari EverandEbstein Anomaly, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsBelum ada peringkat
- Preterm Prelabour Rupture of Membrane, Prelabour RuptureDokumen14 halamanPreterm Prelabour Rupture of Membrane, Prelabour RuptureTengku NorshaherahBelum ada peringkat
- Nephrolithiasis: in The ClinicDokumen16 halamanNephrolithiasis: in The ClinicJohnBelum ada peringkat
- Idiopathic Thrombocytopenic Purpura (ITP)Dokumen7 halamanIdiopathic Thrombocytopenic Purpura (ITP)Rizqka PertiwiBelum ada peringkat
- Ectopic Pregnancy - OMDokumen9 halamanEctopic Pregnancy - OMrheindBelum ada peringkat
- Prenatal Diagnosis Techniques GuideDokumen33 halamanPrenatal Diagnosis Techniques Guidejien_yeenBelum ada peringkat
- Pregnancy Uterus Fetus Embryo: Morbidity Selectively Reduce Multiple PregnancyDokumen4 halamanPregnancy Uterus Fetus Embryo: Morbidity Selectively Reduce Multiple Pregnancynyzgirl17Belum ada peringkat
- Rubella and PregnancyDokumen6 halamanRubella and PregnancyKABERA RENEBelum ada peringkat
- Abruptio PlacentaDokumen5 halamanAbruptio PlacentaJuan Carlo Z. SolidumBelum ada peringkat
- Bladder DiverticulaDokumen23 halamanBladder DiverticulaJeanette CallejasBelum ada peringkat
- Cystitis in Females Clinical Presentation - History, Physical Examination, Acute Urethritis Versus CystitisDokumen6 halamanCystitis in Females Clinical Presentation - History, Physical Examination, Acute Urethritis Versus CystitisotakmesumBelum ada peringkat
- Fetal MonitoringDokumen80 halamanFetal MonitoringNagat Salama100% (1)
- Prenatal ScreeningDokumen61 halamanPrenatal Screeningjoycechicago100% (1)
- Abdominal AssessmentDokumen31 halamanAbdominal Assessmentdbryant0101100% (2)
- CH 10 - Antepartum Fetal AssessmentDokumen8 halamanCH 10 - Antepartum Fetal Assessmentnat0118100% (1)
- Neural Tube Defects: Group 1Dokumen28 halamanNeural Tube Defects: Group 1imneverwrong2492100% (1)
- O&G: Sexually Transmitted InfectionsDokumen3 halamanO&G: Sexually Transmitted InfectionsSok-Moi ChokBelum ada peringkat
- Essential Update: Pediatric Pneumonia May Be Effectively Treated With Twice-Daily AmoxicillinDokumen54 halamanEssential Update: Pediatric Pneumonia May Be Effectively Treated With Twice-Daily AmoxicillinYostesara Maurena SantosaBelum ada peringkat
- Emily B. Baglione CRNA, BSN, MS,: Chief OB CRNA, Anesthesia Group of AlbanyDokumen55 halamanEmily B. Baglione CRNA, BSN, MS,: Chief OB CRNA, Anesthesia Group of AlbanyAsyfiyaTami100% (1)
- Antenatal Care: Physiological Changes in PregnancyDokumen2 halamanAntenatal Care: Physiological Changes in PregnancyAlexander Ennes100% (1)
- PreeclampsiaDokumen14 halamanPreeclampsiaHenny NovitasariBelum ada peringkat
- Situational Analysis of Public Health Nursing Personnel in IndiaDokumen60 halamanSituational Analysis of Public Health Nursing Personnel in IndiaTamilNurse.com100% (1)
- Rheumatic Heart DiseaseDokumen13 halamanRheumatic Heart Diseasedy15Belum ada peringkat
- Abruptio Placenta B-1Dokumen29 halamanAbruptio Placenta B-1drsachinhBelum ada peringkat
- Hypothyroidism in Pregnancy: Causes, Effects and ManagementDokumen29 halamanHypothyroidism in Pregnancy: Causes, Effects and ManagementhanaddulBelum ada peringkat
- Ventricular Septal DefectDokumen8 halamanVentricular Septal DefectMarina RotaruBelum ada peringkat
- Ob SGDDokumen88 halamanOb SGDFerdinand Luis SuarezBelum ada peringkat
- Gestational HypertensionDokumen5 halamanGestational HypertensionJason Jimmy Lee PillayBelum ada peringkat
- The clinical value of blood testsDokumen35 halamanThe clinical value of blood testsAgus SyaifudinBelum ada peringkat
- Pap SmearDokumen3 halamanPap SmearcziehjheyBelum ada peringkat
- Top 10 leading causes of morbidity & mortality in the Philippines in 2007Dokumen7 halamanTop 10 leading causes of morbidity & mortality in the Philippines in 2007Raisa Robelle Quicho100% (1)
- Obstetric Case Study CesarianDokumen16 halamanObstetric Case Study CesarianRazan NasereddineBelum ada peringkat
- COPD Secondaryto PTBDokumen142 halamanCOPD Secondaryto PTBallexiscampaner100% (2)
- Report - For MaamDokumen7 halamanReport - For MaamSherchen Antonio-CortesBelum ada peringkat
- Polycystic Kidney DiseaseDokumen13 halamanPolycystic Kidney DiseaseMadlen212Belum ada peringkat
- Physiology of the Menstrual CycleDokumen6 halamanPhysiology of the Menstrual CyclegmindalanoBelum ada peringkat
- Essential Intrapartum and Newborn Care 1Dokumen5 halamanEssential Intrapartum and Newborn Care 1Genierose YantoBelum ada peringkat
- 6-Health Problems Common in PreschoolerDokumen36 halaman6-Health Problems Common in PreschoolerPam Lala100% (2)
- OB 2.01 High Risk Pregnancy - Prenatal Assessment PDFDokumen10 halamanOB 2.01 High Risk Pregnancy - Prenatal Assessment PDFRaquel ReyesBelum ada peringkat
- Assessing Fetal and Maternal Health: Prenatal Care: Health Promotion During PregnancyDokumen8 halamanAssessing Fetal and Maternal Health: Prenatal Care: Health Promotion During PregnancyMIKAELA DAVIDBelum ada peringkat
- Benign Febril Convulsion PDFDokumen18 halamanBenign Febril Convulsion PDFAESTHETIC PHOTOBelum ada peringkat
- Hypertension in Pregnancy Classification and ManagementDokumen44 halamanHypertension in Pregnancy Classification and ManagementIrfandy Chairi Sulaiman Lubis100% (1)
- Case 9: 2-Week-Old With Lethargy - CrimsonDokumen7 halamanCase 9: 2-Week-Old With Lethargy - Crimsonalwaysbeclosing52Belum ada peringkat
- MENSTRUATION: THE BASICSDokumen56 halamanMENSTRUATION: THE BASICSFev BanataoBelum ada peringkat
- Bleeding DisordersDokumen24 halamanBleeding Disorderskholoud220Belum ada peringkat
- Preeclampsia and EclampsiaDokumen23 halamanPreeclampsia and Eclampsiaapi-3705046100% (6)
- Trichomoniasis: Clinical Manifestations, Diagnosis and ManagementDokumen6 halamanTrichomoniasis: Clinical Manifestations, Diagnosis and ManagementRabecca TobingBelum ada peringkat
- Infants Diabetic MothersDokumen17 halamanInfants Diabetic MothersJaya PrabhaBelum ada peringkat
- HypertensionDokumen6 halamanHypertensionTj Kevin P-DoctorBelum ada peringkat
- Health Education PlanDokumen10 halamanHealth Education PlanJulienne Sanchez-SalazarBelum ada peringkat
- Medical Diseases Complicating Pregnancy: by The Name of AllahDokumen45 halamanMedical Diseases Complicating Pregnancy: by The Name of Allah'محمد علي' محمد لافيBelum ada peringkat
- Clinical Nursing JudgementDokumen6 halamanClinical Nursing Judgementapi-353709602Belum ada peringkat
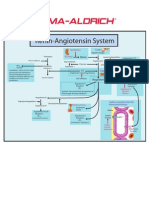
- Renin-Angiotensin SystemDokumen1 halamanRenin-Angiotensin SystemSigma-Aldrich100% (2)
- Normal Postpartum Changes Parameter First 24 H Clinical Heart RateDokumen14 halamanNormal Postpartum Changes Parameter First 24 H Clinical Heart RatemiacajBelum ada peringkat
- Osh State UniversityDokumen14 halamanOsh State Universitykhuzaima9Belum ada peringkat
- Wilm'S Tumor IDokumen25 halamanWilm'S Tumor IBiancaGabatinoAbarca100% (1)
- What is an NCPDokumen38 halamanWhat is an NCPSARAH DIANA ROSE S. MANALILI100% (1)
- PreeclampsiaDokumen4 halamanPreeclampsiairismaronBelum ada peringkat
- 05 DystociaDokumen10 halaman05 DystociaRiantiara PutrizaBelum ada peringkat
- Premature Rupture of MembranesDokumen9 halamanPremature Rupture of MembranesYessica MelianyBelum ada peringkat
- Student study on family health and pregnancy in rural ZimbabweDokumen3 halamanStudent study on family health and pregnancy in rural ZimbabweTubocurareBelum ada peringkat
- Functional Abdominal Cramping Pain Expert Practical Guidance 2022Dokumen9 halamanFunctional Abdominal Cramping Pain Expert Practical Guidance 2022Mohamad MostafaBelum ada peringkat
- From Wikipedia, The Free EncyclopediaDokumen12 halamanFrom Wikipedia, The Free EncyclopediaCharlie EspinoBelum ada peringkat
- Eyelid Eversion and Inversion Causes and TreatmentsDokumen17 halamanEyelid Eversion and Inversion Causes and TreatmentsmanognaaaaBelum ada peringkat
- Clinical Study ReportDokumen5 halamanClinical Study ReportAlexandraCirlanBelum ada peringkat
- Melanoma Cancer PresentationDokumen13 halamanMelanoma Cancer PresentationMerlyn JeejoBelum ada peringkat
- Symposiumbooklet CareerDokumen36 halamanSymposiumbooklet Careerroh009Belum ada peringkat
- Typhoid FeverDokumen52 halamanTyphoid Fevertummalapalli venkateswara rao100% (5)
- Canadian Standards For Hospital LibrariesDokumen4 halamanCanadian Standards For Hospital LibrariesFernando HernandezBelum ada peringkat
- Local Anesthetic Systemic Toxicity AlgorithmDokumen1 halamanLocal Anesthetic Systemic Toxicity AlgorithmSydney JenningsBelum ada peringkat
- Class III Cavity Treatment (Procedure, Materials)Dokumen2 halamanClass III Cavity Treatment (Procedure, Materials)Manos KritikosBelum ada peringkat
- Patch ClampDokumen4 halamanPatch ClampXael GarciaBelum ada peringkat
- Cghs Rates BangaloreDokumen26 halamanCghs Rates Bangaloregr_viswanathBelum ada peringkat
- Surat Izin Masuk: FM.01-AOP - ROM/Rev.4.0/29.01.2020Dokumen4 halamanSurat Izin Masuk: FM.01-AOP - ROM/Rev.4.0/29.01.2020Donking ThotosikBelum ada peringkat
- Endocrine Exam ReviewDokumen2 halamanEndocrine Exam Reviewrockforj3susBelum ada peringkat
- Price Increase 1 January 2020 For Customers VET PDFDokumen9 halamanPrice Increase 1 January 2020 For Customers VET PDFI Dewa made SuwardanaBelum ada peringkat
- JC Oncology55211005Dokumen32 halamanJC Oncology55211005Neenuch ManeenuchBelum ada peringkat
- District: Rajkot Name of Institute: P.D.U. Medical CollegeDokumen9 halamanDistrict: Rajkot Name of Institute: P.D.U. Medical CollegeManas K. TrivediBelum ada peringkat
- PCI-DPharm Syllabus Guidelines 2020Dokumen30 halamanPCI-DPharm Syllabus Guidelines 2020Chander PrakashBelum ada peringkat
- EMTALADokumen5 halamanEMTALAJimmy MillerBelum ada peringkat
- SextafectaDokumen2 halamanSextafectaAndres Felipe Perez SanchezBelum ada peringkat
- Rangkuman by Yulia VionitaDokumen21 halamanRangkuman by Yulia VionitaRizqi AkbarBelum ada peringkat
- Nutrients: Obesity and Dyslipidemia in South AsiansDokumen26 halamanNutrients: Obesity and Dyslipidemia in South AsiansFitriBelum ada peringkat
- Kumara Reiki 2013 Attunement NotesDokumen17 halamanKumara Reiki 2013 Attunement NotesHaryadi Yadi100% (2)
- ANATOMY AND PHYSIOLOGY of RabiesDokumen5 halamanANATOMY AND PHYSIOLOGY of RabiesDavid CalaloBelum ada peringkat
- Ac PolypDokumen18 halamanAc PolypSusmi CmBelum ada peringkat
- Drug Control Policy of BangladeshDokumen51 halamanDrug Control Policy of BangladeshHedayat Ullah33% (3)
- Brochure DiseaseDokumen2 halamanBrochure Diseaseapi-295870217Belum ada peringkat
- Cardiovascular Nursing NotesDokumen17 halamanCardiovascular Nursing NotesLucky GomezBelum ada peringkat
- UrinalysisDokumen43 halamanUrinalysisJames Knowell75% (4)