Anda mungkin juga menyukai
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Introduction To The Philosophy of The Human Person: Quarter II-Module 13: Meaningful LifeDokumen12 halamanIntroduction To The Philosophy of The Human Person: Quarter II-Module 13: Meaningful LifeArien DinoBelum ada peringkat
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- Module 3Dokumen2 halamanModule 3lynel jim malicdem100% (2)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- Kindergarten Science Lesson Plan 1Dokumen12 halamanKindergarten Science Lesson Plan 1api-448771701Belum ada peringkat
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Book List 2023-2024Dokumen3 halamanBook List 2023-2024Valerixal PlayzzBelum ada peringkat
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- Ind Potential SurveyDokumen19 halamanInd Potential SurveyNimish PilankarBelum ada peringkat
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- (Edmond Bordeaux Szekely) Sexual Harmony (B-Ok - CC) PDFDokumen64 halaman(Edmond Bordeaux Szekely) Sexual Harmony (B-Ok - CC) PDFChristopher Carrillo100% (2)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Headway 5th Edition BrochureDokumen6 halamanHeadway 5th Edition BrochureJyothi50% (6)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Pronunciation AssesmentDokumen9 halamanPronunciation AssesmentRaphaela Alencar100% (1)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- What Is TeachingDokumen7 halamanWhat Is TeachingAlexandre Andreatta100% (1)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- Bonafide Certificate NIT RaipurDokumen1 halamanBonafide Certificate NIT RaipurPiyush PastorBelum ada peringkat
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Case Study MobDokumen1 halamanCase Study MobRamamohan ReddyBelum ada peringkat
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Individuals With Disabilities Education ActDokumen33 halamanIndividuals With Disabilities Education ActPiney Martin100% (1)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
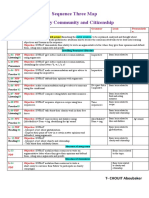
- CHOUIT Aboubaker MS4 Seq03 MapDokumen1 halamanCHOUIT Aboubaker MS4 Seq03 Mapthe rose of snow زهرة الثلج100% (1)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- THPT Đoan HùngDokumen5 halamanTHPT Đoan Hùng04 Nguyễn Ngọc ÁnhBelum ada peringkat
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- Alternative Delivery SystemDokumen10 halamanAlternative Delivery SystemJulieta Busico100% (1)
- The Invisalign SystemDokumen8 halamanThe Invisalign SystemDr Mohammed Nabeel0% (1)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- 123 - Jan-Feb1947 - The Purpose of EducationDokumen2 halaman123 - Jan-Feb1947 - The Purpose of EducationBen LernerBelum ada peringkat
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Syllabus AssignmentDokumen4 halamanSyllabus Assignmentapi-269308807Belum ada peringkat
- Integers - Daily Lesson PlanDokumen5 halamanIntegers - Daily Lesson PlanAmron AzmanBelum ada peringkat
- Fixing Lien of BRCs Upper Primary Working Under SSADokumen2 halamanFixing Lien of BRCs Upper Primary Working Under SSAVIJAY KUMAR HEERBelum ada peringkat
- SEMINAR 08 Agreement and DisagreementDokumen5 halamanSEMINAR 08 Agreement and Disagreementdragomir_emilia92Belum ada peringkat
- ReflectionDokumen4 halamanReflectionNelykah Rianne MartijaBelum ada peringkat
- Cloze Reading ProceduresDokumen7 halamanCloze Reading Proceduresapi-383947273Belum ada peringkat
- Accountant. CVDokumen4 halamanAccountant. CVNamwangala Rashid NatinduBelum ada peringkat
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Teacher ReflectionDokumen3 halamanTeacher Reflectionapi-283337613Belum ada peringkat
- Importance of Cb2Dokumen2 halamanImportance of Cb2Abhinav RanjanBelum ada peringkat
- Kaegi, W - Byzantium Tema 6Dokumen373 halamanKaegi, W - Byzantium Tema 6beatrizBelum ada peringkat
- 4 PillarsDokumen3 halaman4 PillarsMharaTootBelum ada peringkat
- Result at A Glance: Choudhary Charan Singh University, MeerutDokumen11 halamanResult at A Glance: Choudhary Charan Singh University, MeerutParvinder SinghBelum ada peringkat
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- A Critical Analysis of Cultural Content in EFL Materials-A ReimannDokumen17 halamanA Critical Analysis of Cultural Content in EFL Materials-A ReimannJasmina PantićBelum ada peringkat
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)