Anda mungkin juga menyukai
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- CDH Medical & Surgical ManagementDokumen33 halamanCDH Medical & Surgical ManagementBryan Paul RamirezBelum ada peringkat
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- Clinical Trial: Effectiveness of Lactobacillus Rhamnosus (Strains E N, Oxy and Pen) in The Prevention of Antibiotic-Associated Diarrhoea in ChildrenDokumen8 halamanClinical Trial: Effectiveness of Lactobacillus Rhamnosus (Strains E N, Oxy and Pen) in The Prevention of Antibiotic-Associated Diarrhoea in ChildrenBryan Paul RamirezBelum ada peringkat
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Office Orthopaedics: Ramirez, Bryan Paul GDokumen57 halamanOffice Orthopaedics: Ramirez, Bryan Paul GBryan Paul RamirezBelum ada peringkat
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (894)
- Netter's Osteoarthritis R HipDokumen3 halamanNetter's Osteoarthritis R HipBryan Paul RamirezBelum ada peringkat
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Appraisal Form For DiagnosisDokumen3 halamanAppraisal Form For DiagnosisBryan Paul RamirezBelum ada peringkat
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Specific and Social Phobias OCDDokumen19 halamanSpecific and Social Phobias OCDBryan Paul RamirezBelum ada peringkat
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- CMC Protocol DraftDokumen11 halamanCMC Protocol DraftBryan Paul RamirezBelum ada peringkat
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Ortho CMC LabsDokumen1 halamanOrtho CMC LabsBryan Paul RamirezBelum ada peringkat
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- Appd BPDDokumen25 halamanAppd BPDBryan Paul RamirezBelum ada peringkat
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- JI Duty Schedule Psychiatry Sept 1-15, 2011Dokumen1 halamanJI Duty Schedule Psychiatry Sept 1-15, 2011Bryan Paul RamirezBelum ada peringkat
- High-Resolution Ultrasonography of The First Metatarsal Phalangeal JointDokumen55 halamanHigh-Resolution Ultrasonography of The First Metatarsal Phalangeal JointBryan Paul RamirezBelum ada peringkat
- ENTDokumen51 halamanENTBryan Paul Ramirez100% (1)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Plan of Activities June - JulyDokumen13 halamanPlan of Activities June - JulyBryan Paul RamirezBelum ada peringkat
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- Plan of Activites Revised v.3Dokumen28 halamanPlan of Activites Revised v.3Bryan Paul RamirezBelum ada peringkat
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Plan of Activities June - JulyDokumen7 halamanPlan of Activities June - JulyBryan Paul RamirezBelum ada peringkat
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Plan of Activities: Brgy. Batas-DaoDokumen28 halamanPlan of Activities: Brgy. Batas-DaoBryan Paul RamirezBelum ada peringkat
- Introduction To Gerontology and Theories of AgingDokumen106 halamanIntroduction To Gerontology and Theories of AgingCyden Shame delos Santos100% (1)
- First Floor Plan: Covered Area 1028.00 SQ MDokumen1 halamanFirst Floor Plan: Covered Area 1028.00 SQ MNit56122Belum ada peringkat
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Eric Wahlberg, Jerry Goldstone - Emergency Vascular Surgery - A Practical Guide-Springer-Verlag (2017)Dokumen216 halamanEric Wahlberg, Jerry Goldstone - Emergency Vascular Surgery - A Practical Guide-Springer-Verlag (2017)Conțiu Maria Larisa100% (4)
- StiDokumen12 halamanStiValentinaBelum ada peringkat
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Aerobic Dancing BenefitsDokumen4 halamanAerobic Dancing BenefitsDal.giBelum ada peringkat
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- Influenza: Clerk Pineda, Ma. Bernadette BDokumen22 halamanInfluenza: Clerk Pineda, Ma. Bernadette BMa. Bernadette PinedaBelum ada peringkat
- Colorful insights into mental wellnessDokumen4 halamanColorful insights into mental wellnessJonrheym RemegiaBelum ada peringkat
- Nursing ApplicationDokumen1 halamanNursing ApplicationGuru JiBelum ada peringkat
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- (IU-GADSOP 2018) (A4) First Announcement - Versi ADokumen1 halaman(IU-GADSOP 2018) (A4) First Announcement - Versi AIfah Inayah D'zatrichaBelum ada peringkat
- Advantage and DisadvantageDokumen5 halamanAdvantage and Disadvantageحسين يوسفBelum ada peringkat
- A Clinical Pathway To Standardize Care of Children With Delirium in Pediatric Inpatient Settings-2019Dokumen10 halamanA Clinical Pathway To Standardize Care of Children With Delirium in Pediatric Inpatient Settings-2019Juan ParedesBelum ada peringkat
- What Vaccines Do BC Adults NeedDokumen2 halamanWhat Vaccines Do BC Adults NeedCatalina VisanBelum ada peringkat
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Medicolegal Tips For DoctorsDokumen10 halamanMedicolegal Tips For DoctorsFajar NarakusumaBelum ada peringkat
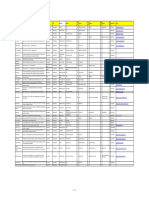
- Name Clinic/Hosp/Med Name &address Area City Speciality SEWA01 Disc 01 SEWA02 DIS C02 SEWA03 Disc 03 SEWA04 DIS C04 Contact No. EmailDokumen8 halamanName Clinic/Hosp/Med Name &address Area City Speciality SEWA01 Disc 01 SEWA02 DIS C02 SEWA03 Disc 03 SEWA04 DIS C04 Contact No. EmailshrutiBelum ada peringkat
- Secondary Survey for Trauma PatientsDokumen18 halamanSecondary Survey for Trauma PatientsJohn BrittoBelum ada peringkat
- Additional Vacancies at CHCs in Health and Family Welfare Services For One Year Government ServicesDokumen5 halamanAdditional Vacancies at CHCs in Health and Family Welfare Services For One Year Government ServicesBhavvBelum ada peringkat
- 2 Conversion of Iv To PoDokumen27 halaman2 Conversion of Iv To PoSreya Sanil100% (1)
- Jackson Baumgartner ResumeDokumen2 halamanJackson Baumgartner Resumeapi-399299717Belum ada peringkat
- ICH E2E GuidelineDokumen20 halamanICH E2E Guidelinetito1628Belum ada peringkat
- Clinical Pharmacology Answers 2022Dokumen223 halamanClinical Pharmacology Answers 2022nancy voraBelum ada peringkat
- The Hall Technique: Food for ThoughtDokumen50 halamanThe Hall Technique: Food for ThoughtMustafa Tambawala100% (1)
- Nanotechnology Based Drug Delivery System,: "Nanomedicine"Dokumen10 halamanNanotechnology Based Drug Delivery System,: "Nanomedicine"rohit a bhosaleBelum ada peringkat
- 3M Mask and AntisepticDokumen2 halaman3M Mask and AntisepticДимитър ПетровBelum ada peringkat
- Bum Run GradDokumen10 halamanBum Run GradsabyasachiBelum ada peringkat
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- DDR PrimeDokumen4 halamanDDR PrimeNona AlyBelum ada peringkat
- CPG Management of Dementia (2nd Edition)Dokumen162 halamanCPG Management of Dementia (2nd Edition)umiraihana1Belum ada peringkat
- What Is ExerciseDokumen3 halamanWhat Is ExerciseJehada AbdukadilBelum ada peringkat
- Asthma Word Fill KeyDokumen2 halamanAsthma Word Fill KeyKaren brooksBelum ada peringkat
- Closing Event For Surrey Perinatal Impact PartnershipDokumen11 halamanClosing Event For Surrey Perinatal Impact Partnershipranjanadas0% (1)
- Contingency Plan For Covid 19Dokumen27 halamanContingency Plan For Covid 19Oteee17Belum ada peringkat
- The Age of Magical Overthinking: Notes on Modern IrrationalityDari EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityPenilaian: 4 dari 5 bintang4/5 (13)