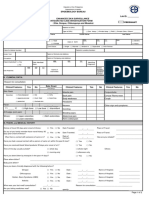
BREAST CANCER DETECTION AND CARE
REQUEST FOR MASTOGRAPHY
FOLIO
I. Unit identification II.Date of application
day month year
Medical Unit _________________ Delegation _____________________ Jurisdiction ______________
III. Patient identification
No.Affiliation|CURP ___________ _______|| ________Office ____________ M V
_______ year
Name ____________________ ________________ Age
Paternal Surname s
Mother's Last Name Name(s)
Address
Street and Colony
number I I I I I I I or Tel
Municipality or Delegation State Zip Code
IV. Clinical Examination Results_______V.History
of mastography [1] Yes No. [2]No
[1] Normal [2] Abnormal 5.2 Date of the last rm mastography
day month year
Name, Category and
Applicant's signature ___________________________________________ Enrollment:______________
RESULTS
VI. Date of mastography VII. Radiologic Technician Registration_____________
day month year
VIII. Quality of mastography IX. Date of interpretation rm
day month year
[ ] Full breast image [Nipple perpendicular to the breast [ ] Adequate compression
Symmetric breast images [ ] Appropriate exposure [ ] Inadequate for
interpretation [ ] Inadequate for interpretation
X. Radiological findings D I
If inadequate, specify the cause
DI
[asymmetric BREAST DENSITY oo
o o [ ] NODULE OR MASS
[ALMOST ENTIRELY FATTY (< 25% FIBROGLANDULAR) SHAPE__________________
[DISPERSED FIBROGLANDULAR ( 25-50% FIBROGLANDULAR) SIZE_____________CM
[ ] HETEROGENEOUS (51-75% FIBROGLANDULAR) [microcalcifications
[EXTREMELY DENSE (<75% FIBROGLANDULAR) [ ] MACROCALCIFICATIONS
XI.Diagnosis (BIRADS) DI
[ 0] INCONCLUSIVE STUDY [ 1] [3] PROBABLY BENIGN
NORMAL BREAST [ 2] BENIGN [4] PROBABLY MALIGNANT
FINDINGS [ 1] NORMAL BREAST [ 2] [5] MALIGNANT FINDINGS
BENIGN FINDINGS
Remarks
XII. Conduct to be followed
[ 1] Detection in two years [3] Evaluation in a short time (6 months)
[ 2] Repeat mastography due to technical failure [4] Reference for diagnostic evaluation
XII. Name and signature of radiologist__________________________ Enrollment:_______________
XIV. Report the result to the woman XV. Reference 1.5.1 Date
day month year
Illi 1.5.2 Unit _______________ Delegation_______________
day month year
Anda mungkin juga menyukai
- Clinical Face Sheet: - A.M. - P.M. - A.M. - P.MDokumen15 halamanClinical Face Sheet: - A.M. - P.M. - A.M. - P.MNikitaCaitlynLeyaleyBelum ada peringkat
- Patients Chart For StudentsDokumen18 halamanPatients Chart For StudentsRyrey Abraham PacamanaBelum ada peringkat
- Case Investigation Forms - Pidsrmop3ed 1Dokumen16 halamanCase Investigation Forms - Pidsrmop3ed 1RHU Dupax del Sur100% (3)
- Imm Golden Points by DR Hameed DawarDokumen15 halamanImm Golden Points by DR Hameed DawarUsama1987Belum ada peringkat
- CHN Survey FormDokumen5 halamanCHN Survey FormPʀɩŋcɘss LɩʌBelum ada peringkat
- Central Nervous System Tumours: WHO Classification of Tumours - 5th EditionDokumen584 halamanCentral Nervous System Tumours: WHO Classification of Tumours - 5th EditionSamira KhalilBelum ada peringkat
- Chikungunya FormDokumen2 halamanChikungunya FormTin Causaren-Gertos100% (1)
- Furuno FMD ECDIS PDFDokumen14 halamanFuruno FMD ECDIS PDFScribdTranslations100% (1)
- 1 1 MFI Survey QuestionnaireDokumen26 halaman1 1 MFI Survey QuestionnaireAbhishek Singh75% (4)
- Personalizing Precision Medicine: A Global Voyage from Vision to RealityDari EverandPersonalizing Precision Medicine: A Global Voyage from Vision to RealityPenilaian: 5 dari 5 bintang5/5 (2)
- Cif Zika - 2016 PDFDokumen3 halamanCif Zika - 2016 PDFNicholai CabadduBelum ada peringkat
- Medical Attendants Certificate17062019Dokumen2 halamanMedical Attendants Certificate17062019PrathameshBelum ada peringkat
- NDMU DR GuideDokumen5 halamanNDMU DR GuideInsatiable CleeBelum ada peringkat
- Clinical Face Sheet: Category of PatientDokumen14 halamanClinical Face Sheet: Category of PatientMarjorie UmipigBelum ada peringkat
- Measles Case Reporting Form I.Case Identification/ Demographic DetailsDokumen2 halamanMeasles Case Reporting Form I.Case Identification/ Demographic DetailsActivity ManagerBelum ada peringkat
- Kenyan Medical CertificateDokumen3 halamanKenyan Medical CertificateIsrael JacksonBelum ada peringkat
- Animal Bite Treatment RecordDokumen2 halamanAnimal Bite Treatment RecordDariel Baculbas AlvarezBelum ada peringkat
- Nursing Seminar 1 SAS Session 14Dokumen8 halamanNursing Seminar 1 SAS Session 14ZiaBelum ada peringkat
- Case Report Form For HFMDDokumen2 halamanCase Report Form For HFMDMendez RhuBelum ada peringkat
- CRF HFMD AsmghDokumen2 halamanCRF HFMD AsmghRyeowook RyeBelum ada peringkat
- English For Academic and Professional Purposes Final Examination OCTOBER - , 2017 FIRST SEMESTER S.Y. 2017-2018Dokumen4 halamanEnglish For Academic and Professional Purposes Final Examination OCTOBER - , 2017 FIRST SEMESTER S.Y. 2017-2018Kristel EbradaBelum ada peringkat
- National Nutrition Council P2Dokumen1 halamanNational Nutrition Council P2RANDY BAOGBOGBelum ada peringkat
- CIF-MR 2022 Ver1Dokumen2 halamanCIF-MR 2022 Ver1Ivy marie BonBelum ada peringkat
- Diversion ContractDokumen8 halamanDiversion ContractMaricho BentazalBelum ada peringkat
- Max Life Insurance Company Limited Tumor Questionnaire: CheekDokumen3 halamanMax Life Insurance Company Limited Tumor Questionnaire: CheekDharma GnaniBelum ada peringkat
- Measles CIF 2014Dokumen2 halamanMeasles CIF 2014RionaMarieMagbutayBelum ada peringkat
- Pages 5 Form FDokumen2 halamanPages 5 Form FANIL KUMARBelum ada peringkat
- HPV Template MasterlistDokumen1 halamanHPV Template Masterlistmarialovella.gonzagaBelum ada peringkat
- 5 Assesed WoredaDokumen59 halaman5 Assesed WoredaatakltigebertsadikBelum ada peringkat
- 7 Unassesed Woreda Copy111Dokumen72 halaman7 Unassesed Woreda Copy111atakltigebertsadikBelum ada peringkat
- Clinical Face Sheet: - A.M. - P.M. - A.M. - P.MDokumen16 halamanClinical Face Sheet: - A.M. - P.M. - A.M. - P.MCezanne CruzBelum ada peringkat
- Group Medical Insurance Claim Form Section 2Dokumen1 halamanGroup Medical Insurance Claim Form Section 2Aditya SharmaBelum ada peringkat
- Republic of The Philippines Professional Regulation Commission Board of NursingDokumen7 halamanRepublic of The Philippines Professional Regulation Commission Board of NursingrcaraigBelum ada peringkat
- Application Form Lto Birthing HomeDokumen19 halamanApplication Form Lto Birthing Homemondirah pandaBelum ada peringkat
- Statform3: Republic of The Philippines Department of Health ManilaDokumen10 halamanStatform3: Republic of The Philippines Department of Health ManilaErica WareBelum ada peringkat
- Clinical Face Sheet: - A.M. - P.M. - A.M. - P.MDokumen11 halamanClinical Face Sheet: - A.M. - P.M. - A.M. - P.M3B NOVIDA, ALEYA G.Belum ada peringkat
- (Pink) /merah Muda Victim Identification Form/ B0: Jenis Bencana Tempat Bencana Tanggal BencanaDokumen21 halaman(Pink) /merah Muda Victim Identification Form/ B0: Jenis Bencana Tempat Bencana Tanggal BencanaUsbahBelum ada peringkat
- Epilepsy Questionnaire For Proposed Insured/OwnerDokumen1 halamanEpilepsy Questionnaire For Proposed Insured/OwnerSincerely ReynBelum ada peringkat
- Zika IcifDokumen2 halamanZika IcifMarav SymbBelum ada peringkat
- New Enhanced Zika CIFDokumen3 halamanNew Enhanced Zika CIFMarav SymbBelum ada peringkat
- FORM F NewDokumen2 halamanFORM F NewNilesh Ghadge50% (2)
- Format of Authorization Application For PHC and DispensaryDokumen7 halamanFormat of Authorization Application For PHC and DispensaryRajat AroraBelum ada peringkat
- Anthrax CifDokumen2 halamanAnthrax CifMary Anne Grace GarridoBelum ada peringkat
- 3rd Monthly ExaminationDokumen10 halaman3rd Monthly ExaminationJay Cariel GastonesBelum ada peringkat
- Hypertension Questionnaire For Proposed Insured/OwnerDokumen1 halamanHypertension Questionnaire For Proposed Insured/OwnerSincerely ReynBelum ada peringkat
- Borang Medical Card-Dhamir ImranDokumen7 halamanBorang Medical Card-Dhamir ImranaimannrezzBelum ada peringkat
- Annex 1Dokumen3 halamanAnnex 1Saroj PokhrelBelum ada peringkat
- NPMP Parivar Proposal FormDokumen8 halamanNPMP Parivar Proposal Formpradip nathujiBelum ada peringkat
- Course Registration FormDokumen3 halamanCourse Registration Formmusinguzi albertBelum ada peringkat
- ReimbursementFormA BDokumen5 halamanReimbursementFormA BSupriya KandukuriBelum ada peringkat
- Anthem Medical Claim FormDokumen2 halamanAnthem Medical Claim FormsaiprojectworkBelum ada peringkat
- CIF-Meningococcal DiseaseDokumen2 halamanCIF-Meningococcal DiseaseIvy marie BonBelum ada peringkat
- UoI Diploma Joining Instruction 2020 21Dokumen4 halamanUoI Diploma Joining Instruction 2020 21Haason TzBelum ada peringkat
- Case History ExamDokumen12 halamanCase History ExamAnudnya JadhavBelum ada peringkat
- Case Investigation Form - Measles-RubellaDokumen2 halamanCase Investigation Form - Measles-Rubellaclaverialc10Belum ada peringkat
- Recording Form 1: Masterlist of Grade 1 Students: School-Based ImmunizationDokumen1 halamanRecording Form 1: Masterlist of Grade 1 Students: School-Based ImmunizationJesse100% (1)
- PRC Form (Minor Operation)Dokumen1 halamanPRC Form (Minor Operation)mawelBelum ada peringkat
- Revised Preauth Form IRDADokumen5 halamanRevised Preauth Form IRDASurbhi SinghBelum ada peringkat
- PRC-Assisted Delivery 2010Dokumen1 halamanPRC-Assisted Delivery 2010mawelBelum ada peringkat
- 45 - PG 42Dokumen1 halaman45 - PG 42api-235687879Belum ada peringkat
- NYCIntlProgramsAppForm - LastName, FirstNameDokumen3 halamanNYCIntlProgramsAppForm - LastName, FirstNamePau SantosBelum ada peringkat
- Attendance For Barangay AssemblyDokumen4 halamanAttendance For Barangay Assemblycbtercero22Belum ada peringkat
- CIF RotavirusDokumen1 halamanCIF RotavirusIvy marie BonBelum ada peringkat
- Administration Financière t2 UPNDokumen10 halamanAdministration Financière t2 UPNScribdTranslationsBelum ada peringkat
- DD124 Exam 2Dokumen7 halamanDD124 Exam 2ScribdTranslationsBelum ada peringkat
- Aa Preventive Maintenance Report - ItpDokumen32 halamanAa Preventive Maintenance Report - ItpScribdTranslationsBelum ada peringkat
- Case Study - Solution - Alternative FinancingDokumen6 halamanCase Study - Solution - Alternative FinancingScribdTranslationsBelum ada peringkat
- Case 4 ASICS QuestionsDokumen1 halamanCase 4 ASICS QuestionsScribdTranslationsBelum ada peringkat
- Final Exam - Financial Administration - Group N°11Dokumen9 halamanFinal Exam - Financial Administration - Group N°11ScribdTranslationsBelum ada peringkat
- Concept Map T8.2Dokumen2 halamanConcept Map T8.2ScribdTranslationsBelum ada peringkat
- Rpas Exam Syllabus SOLVED - WordDokumen9 halamanRpas Exam Syllabus SOLVED - WordScribdTranslationsBelum ada peringkat
- Network Layers ExplanationDokumen3 halamanNetwork Layers ExplanationScribdTranslationsBelum ada peringkat
- Session My Name Is Special and UniqueDokumen2 halamanSession My Name Is Special and UniqueScribdTranslationsBelum ada peringkat
- Workshop 13 Situations Requirements HSEQDokumen14 halamanWorkshop 13 Situations Requirements HSEQScribdTranslationsBelum ada peringkat
- PC3 Simulation Tools For Decision MakingDokumen9 halamanPC3 Simulation Tools For Decision MakingScribdTranslationsBelum ada peringkat
- M2 - TI - Skills For Oral and Written Communication PDFDokumen5 halamanM2 - TI - Skills For Oral and Written Communication PDFScribdTranslationsBelum ada peringkat
- EXCEL PracticeDokumen10 halamanEXCEL PracticeScribdTranslationsBelum ada peringkat
- Coca Cola Performance EvaluationDokumen1 halamanCoca Cola Performance EvaluationScribdTranslationsBelum ada peringkat
- Colun Market ResearchDokumen9 halamanColun Market ResearchScribdTranslationsBelum ada peringkat
- Bank Questions PC Virtual Unit 2Dokumen13 halamanBank Questions PC Virtual Unit 2ScribdTranslationsBelum ada peringkat
- Risk Matrix Going On African Photo SafariDokumen15 halamanRisk Matrix Going On African Photo SafariScribdTranslationsBelum ada peringkat
- Final Work - Applied Statistics For Business.Dokumen28 halamanFinal Work - Applied Statistics For Business.ScribdTranslationsBelum ada peringkat
- Final Work Caixabank CaseDokumen7 halamanFinal Work Caixabank CaseScribdTranslationsBelum ada peringkat
- Exercises and ProblemsDokumen65 halamanExercises and ProblemsScribdTranslationsBelum ada peringkat
- Response To Demand Rendering of Accounts.Dokumen9 halamanResponse To Demand Rendering of Accounts.ScribdTranslationsBelum ada peringkat
- Legal Analysis of George OrwellsDokumen10 halamanLegal Analysis of George OrwellsScribdTranslationsBelum ada peringkat
- Solved T-Student Distribution ExercisesDokumen4 halamanSolved T-Student Distribution ExercisesScribdTranslationsBelum ada peringkat
- SEQUENCE The Process of Construction of The Argentine National State (1853-1880) - 6th MODIFIEDDokumen13 halamanSEQUENCE The Process of Construction of The Argentine National State (1853-1880) - 6th MODIFIEDScribdTranslationsBelum ada peringkat
- Final Questionnaire Module 2 CNDH Prevention of TortureDokumen7 halamanFinal Questionnaire Module 2 CNDH Prevention of TortureScribdTranslationsBelum ada peringkat
- Final Questionnaire Module 1 CNDH Prevention of TortureDokumen5 halamanFinal Questionnaire Module 1 CNDH Prevention of TortureScribdTranslationsBelum ada peringkat
- Life Center - Worthy Are You - Forever PDFDokumen1 halamanLife Center - Worthy Are You - Forever PDFScribdTranslationsBelum ada peringkat
- TaskDokumen2 halamanTaskScribdTranslationsBelum ada peringkat
- Types of DeathDokumen2 halamanTypes of DeathRamseena Udayakumar100% (1)
- GERD Gastroesophageal Reflux Disease Fact SheetDokumen2 halamanGERD Gastroesophageal Reflux Disease Fact SheetFatimah FadilahBelum ada peringkat
- Clinical Presentation, Diagnosis, and Staging of Bladder Cancer - UpToDateDokumen29 halamanClinical Presentation, Diagnosis, and Staging of Bladder Cancer - UpToDateMario Lopez CastellanosBelum ada peringkat
- NCM106-Cellular Aberrations-Module1-Lesson 1Dokumen9 halamanNCM106-Cellular Aberrations-Module1-Lesson 1Esmareldah Henry SirueBelum ada peringkat
- BiologyDokumen14 halamanBiologyKanish KumarBelum ada peringkat
- 10 Penyakit Terbanyak Di Rawat Jalan Di Puskesmas Provinsi Dki Jakarta TW I Tahun 2019Dokumen9 halaman10 Penyakit Terbanyak Di Rawat Jalan Di Puskesmas Provinsi Dki Jakarta TW I Tahun 2019Klinik pratama Iqra' medical centreBelum ada peringkat
- An Essay On Why Your Mouth MattersDokumen5 halamanAn Essay On Why Your Mouth Mattersokeremiriam2020Belum ada peringkat
- Principles of Radiation OncologyDokumen22 halamanPrinciples of Radiation OncologyGina RBelum ada peringkat
- Princess NCP COPDDokumen3 halamanPrincess NCP COPDPrincess Faniega SugatonBelum ada peringkat
- MyxedemaDokumen16 halamanMyxedemaalaamedBelum ada peringkat
- NSTP Common Module 2 Drug EducationDokumen33 halamanNSTP Common Module 2 Drug EducationMerylle Shayne GustiloBelum ada peringkat
- Bhagwanbloodreport - 23 - 888071pdf (2) - 230719 - 065846Dokumen1 halamanBhagwanbloodreport - 23 - 888071pdf (2) - 230719 - 065846Ajay SinghBelum ada peringkat
- Whitbourne7e IM Ch09Dokumen10 halamanWhitbourne7e IM Ch09Antônio Malvar Martins NetoBelum ada peringkat
- Poster SubmissionDokumen1 halamanPoster SubmissionBavadharani MBelum ada peringkat
- Sample # 1 of Latest CK UW Notes-2022Dokumen167 halamanSample # 1 of Latest CK UW Notes-2022Fareena KhanBelum ada peringkat
- WT OetDokumen13 halamanWT OetRomana PereiraBelum ada peringkat
- What Is Newborn ScreeningDokumen2 halamanWhat Is Newborn ScreeningroksanmiBelum ada peringkat
- Clinical Chemistry Tumor MarkersDokumen6 halamanClinical Chemistry Tumor Markerskatherineanne.diamanteBelum ada peringkat
- Drugs of Diabettes: Submitted To Ma'am Maira Riaz. Subject Pharmacy. Submitted By: Group No.9 MembersDokumen21 halamanDrugs of Diabettes: Submitted To Ma'am Maira Riaz. Subject Pharmacy. Submitted By: Group No.9 Membersshizzaarif28Belum ada peringkat
- Anti Phospholipid Syndrome What's New?: Kanadi SumapradjaDokumen22 halamanAnti Phospholipid Syndrome What's New?: Kanadi SumapradjafistyaelchBelum ada peringkat
- Diagnosis and Treatment of Cerebral Venous.10Dokumen21 halamanDiagnosis and Treatment of Cerebral Venous.10Ivan MihailovicBelum ada peringkat
- Biology, Clinical Manifestations, and Treatment of CancerDokumen48 halamanBiology, Clinical Manifestations, and Treatment of CancerNita AndiniBelum ada peringkat
- Academic Year: 2021/2022 Semester: Fall 2021Dokumen27 halamanAcademic Year: 2021/2022 Semester: Fall 2021Marwa abbassBelum ada peringkat
- Drug StudyDokumen4 halamanDrug StudyJessica GlitterBelum ada peringkat
- Full Psych DB InterviewDokumen30 halamanFull Psych DB InterviewAdam GBelum ada peringkat
- Epidemiology and Factors Related To The Survival of Metastatic Kidney Cancers: Retrospective Study at The Mohamed VI Center For The Cancer Treatment in Casablanca, MoroccoDokumen5 halamanEpidemiology and Factors Related To The Survival of Metastatic Kidney Cancers: Retrospective Study at The Mohamed VI Center For The Cancer Treatment in Casablanca, MoroccoInternational Journal of Innovative Science and Research TechnologyBelum ada peringkat
- Jama Schlapbach 2024 Oi 240002 1705616415.31602Dokumen10 halamanJama Schlapbach 2024 Oi 240002 1705616415.31602Laura Alejandra Torres CanchalaBelum ada peringkat
- MCQ in OtologyDokumen6 halamanMCQ in OtologyWael ShamyBelum ada peringkat