Anda mungkin juga menyukai
- Respiratory Care Anatomy and Physiology 3rd Edition Will Beachey Test BankDokumen12 halamanRespiratory Care Anatomy and Physiology 3rd Edition Will Beachey Test BankOcean0% (1)
- General Zoology SyllabusDokumen4 halamanGeneral Zoology SyllabusNL R Q DO100% (3)
- Test Bank For Respiratory Disease A Case Study Approach To Patient Care 3rd Edition by WilkinsDokumen10 halamanTest Bank For Respiratory Disease A Case Study Approach To Patient Care 3rd Edition by Wilkinsa498226706Belum ada peringkat
- Cheatsheet 2Dokumen1 halamanCheatsheet 2Rick Frea86% (7)
- Bilevel VentilationDokumen18 halamanBilevel VentilationBonehead7Belum ada peringkat
- RT Student CRT Entry Exam Review QuestionsDokumen71 halamanRT Student CRT Entry Exam Review QuestionsRenita Washington100% (4)
- Respiratory DysfunctionDokumen1 halamanRespiratory Dysfunctionoxidalaj100% (3)
- CRT Test BanksDokumen257 halamanCRT Test BanksRain Catan Gagarra Saquin100% (2)
- Respiratory Care Review: An Intense Look at Respiratory Care Through Case StudiesDari EverandRespiratory Care Review: An Intense Look at Respiratory Care Through Case StudiesBelum ada peringkat
- 33 Airway ManagementDokumen19 halaman33 Airway ManagementTiffany Helmes100% (2)
- Emergency Room Aerosolized Medication ProtocolDokumen3 halamanEmergency Room Aerosolized Medication ProtocolRick Frea67% (3)
- ABG Practice Problems For N304Dokumen4 halamanABG Practice Problems For N304dlneisha61100% (2)
- Ventilation For DummiesDokumen39 halamanVentilation For Dummiessuyalamit100% (6)
- Cheatsheet 5Dokumen1 halamanCheatsheet 5Rick Frea80% (5)
- Ecg MCQSDokumen2 halamanEcg MCQSZafar Iqbal Manj100% (2)
- Neo-Peds Intubation Cheat SheetDokumen1 halamanNeo-Peds Intubation Cheat SheetRick FreaBelum ada peringkat
- RT ConsultDokumen5 halamanRT ConsultRick Frea100% (2)
- TMCQuestions AllocationDokumen2 halamanTMCQuestions AllocationMyra BuellaBelum ada peringkat
- Respiratory Alkalosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDari EverandRespiratory Alkalosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsBelum ada peringkat
- Acute Respiratory Distress Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDari EverandAcute Respiratory Distress Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsBelum ada peringkat
- Respiratory Failure, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDari EverandRespiratory Failure, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsBelum ada peringkat
- A Simple Guide to Pneumothorax (Collapsed Lungs), Diagnosis, Treatment and Related ConditionsDari EverandA Simple Guide to Pneumothorax (Collapsed Lungs), Diagnosis, Treatment and Related ConditionsBelum ada peringkat
- A Simple Guide to Circulatory Shock, Diagnosis, Treatment and Related ConditionsDari EverandA Simple Guide to Circulatory Shock, Diagnosis, Treatment and Related ConditionsBelum ada peringkat
- Tidal Volumes Cheat SheetDokumen1 halamanTidal Volumes Cheat SheetRick Frea100% (1)
- 99 TMCPractice QuestionsDokumen31 halaman99 TMCPractice QuestionsGustavo OlguinBelum ada peringkat
- Pulmonary Function TestsDokumen9 halamanPulmonary Function TestsRick Frea0% (1)
- Respiratory Therapy: 66 Test Questions Student Respiratory Therapists Get Wrong Every Time: (Volume 2 of 2): Now You Don't Have Too!: Respiratory Therapy Board Exam Preparation, #2Dari EverandRespiratory Therapy: 66 Test Questions Student Respiratory Therapists Get Wrong Every Time: (Volume 2 of 2): Now You Don't Have Too!: Respiratory Therapy Board Exam Preparation, #2Belum ada peringkat
- Emergency in Respiratory Medicine HandbookDokumen73 halamanEmergency in Respiratory Medicine HandbookIndra MahaputraBelum ada peringkat
- Respiratory PharmacologyDokumen12 halamanRespiratory PharmacologywahyudhanapermanaBelum ada peringkat
- Respiratory Medications for Asthma and COPDDokumen20 halamanRespiratory Medications for Asthma and COPDDJJ100% (1)
- Static Compliance & RSBI CheatsheetDokumen1 halamanStatic Compliance & RSBI CheatsheetRick FreaBelum ada peringkat
- Fundamentals Study GuideDokumen37 halamanFundamentals Study GuideGustavo OlguinBelum ada peringkat
- Updated: Dec 07, 2016 Author: Justina Gamache, MD Chief Editor: Guy W Soo Hoo, MD, MPHDokumen42 halamanUpdated: Dec 07, 2016 Author: Justina Gamache, MD Chief Editor: Guy W Soo Hoo, MD, MPHgita suci arianiBelum ada peringkat
- Registered Respiratory TherapistDokumen3 halamanRegistered Respiratory Therapistapi-76909521Belum ada peringkat
- RT!: Reflections on a Career in Respiratory TherapyDari EverandRT!: Reflections on a Career in Respiratory TherapyPenilaian: 3 dari 5 bintang3/5 (1)
- Mechanical Ventilator Management ProtocolDokumen3 halamanMechanical Ventilator Management ProtocolRick Frea100% (2)
- End Tidal Co2Dokumen38 halamanEnd Tidal Co2brentupdegraffBelum ada peringkat
- Respiratory Therapy: 66 Test Questions Student Respiratory Therapists Get Wrong Every Time: (Volume 1 of 2): Now You Don't Have Too!: Respiratory Therapy Board Exam Preparation, #1Dari EverandRespiratory Therapy: 66 Test Questions Student Respiratory Therapists Get Wrong Every Time: (Volume 1 of 2): Now You Don't Have Too!: Respiratory Therapy Board Exam Preparation, #1Belum ada peringkat
- Lower Respiratory Study SheetDokumen13 halamanLower Respiratory Study SheetJune Rhoades100% (2)
- Respiratory PathophysDokumen1 halamanRespiratory PathophysTori IkeharaBelum ada peringkat
- Extubation CriteriaDokumen17 halamanExtubation CriteriaOliver TabagBelum ada peringkat
- Pulmonary Function Test, JARA CSUDokumen73 halamanPulmonary Function Test, JARA CSUJohn NicoleBelum ada peringkat
- Respiratory Therapy FormulasDokumen3 halamanRespiratory Therapy Formulasrtman50% (2)
- Mechanical Ventilation FinalDokumen46 halamanMechanical Ventilation FinalNaven ScorpBelum ada peringkat
- Ecgs Made Easy 5th Edition Aehlert Test BankDokumen14 halamanEcgs Made Easy 5th Edition Aehlert Test BankQuinn50% (2)
- Adjusting Ventilator SettingsDokumen7 halamanAdjusting Ventilator SettingsSiva RamanBelum ada peringkat
- EXAM RRTCheatSheetBookDokumen22 halamanEXAM RRTCheatSheetBookGustavo Olguin100% (2)
- RRT PT AssessmentDokumen39 halamanRRT PT AssessmentRam NasaluddinBelum ada peringkat
- Inhaler LexiconDokumen4 halamanInhaler LexiconRick Frea100% (2)
- Neonatal Resuscitation ProgramDokumen6 halamanNeonatal Resuscitation ProgramRick Frea100% (5)
- Respiratory Disease Symptoms and SignsDokumen2 halamanRespiratory Disease Symptoms and Signstotallyfakeusername100% (1)
- Respiratory Therapy Cave - Ventilator Graphics Cheat SheetDokumen2 halamanRespiratory Therapy Cave - Ventilator Graphics Cheat SheetMarwa El-DegwiBelum ada peringkat
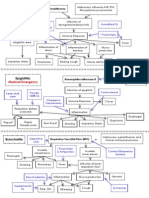
- Classification and Pathophysiology of Respiratory DiseasesDokumen8 halamanClassification and Pathophysiology of Respiratory DiseasesTONY GO AWAYBelum ada peringkat
- Ventilator Modes Study GuideDokumen34 halamanVentilator Modes Study GuideRyn ShadowBelum ada peringkat
- 5 Patient Assessment Skills To Crush The TMC-RRT ExamDokumen4 halaman5 Patient Assessment Skills To Crush The TMC-RRT ExamNaser Abdulfatah Al Hazmi100% (1)
- Respiratory QuizDokumen32 halamanRespiratory Quiztajamulhussainshah0% (1)
- ABG PracticeDokumen16 halamanABG Practiceadni_wg100% (1)
- Board Exam Prep: Essential Tips for SuccessDokumen108 halamanBoard Exam Prep: Essential Tips for SuccessAnonymous FvUBZa100% (1)
- EXAM RRTPracticeQuestionsDokumen30 halamanEXAM RRTPracticeQuestionsGustavo OlguinBelum ada peringkat
- Anesthesia For The Pet Practitioner (2011 3rd Edition)Dokumen216 halamanAnesthesia For The Pet Practitioner (2011 3rd Edition)Amela Dolittle Halilbašić100% (5)
- Overview of Complications Occurring in The Post-Anesthesia Care UnitDokumen14 halamanOverview of Complications Occurring in The Post-Anesthesia Care UnitShahabuddin ShaikhBelum ada peringkat
- Meridians and Points PDFDokumen35 halamanMeridians and Points PDFHamdon Hamad100% (9)
- 3.03 Understand Structures, Functions and Disorders of The Nervous SystemDokumen38 halaman3.03 Understand Structures, Functions and Disorders of The Nervous SystemLoriwinchesterBelum ada peringkat
- Francisco Aboitiz (Auth.) - A Brain For Speech - A View From Evolutionary Neuroanatomy-Palgrave Macmillan UK (2017)Dokumen515 halamanFrancisco Aboitiz (Auth.) - A Brain For Speech - A View From Evolutionary Neuroanatomy-Palgrave Macmillan UK (2017)TecuitlatlBelum ada peringkat
- Abdominal SurgeryDokumen166 halamanAbdominal SurgeryIndera VyasBelum ada peringkat
- Amniodarone (Norvasc) Drug SummDokumen1 halamanAmniodarone (Norvasc) Drug SummWarrenBelum ada peringkat
- Effects of Electromagnetic Forces of Earth On HumansDokumen6 halamanEffects of Electromagnetic Forces of Earth On HumansArtist MetuBelum ada peringkat
- Doppler US Validates Portal Vein Flow in CirrhosisDokumen5 halamanDoppler US Validates Portal Vein Flow in CirrhosisL0v3B00k5Belum ada peringkat
- ECG Interpretation For ACLSDokumen27 halamanECG Interpretation For ACLSZH. omg sarBelum ada peringkat
- Altered Body TemperatureDokumen27 halamanAltered Body TemperatureAnusikta PandaBelum ada peringkat
- CSIR UGC JRF Subjetive Model Test PaperDokumen17 halamanCSIR UGC JRF Subjetive Model Test PaperManu Mallahalli ShanthappaBelum ada peringkat
- BioSignature Review - Are Hormones The Key To Weight LossDokumen19 halamanBioSignature Review - Are Hormones The Key To Weight LossVladimir OlefirenkoBelum ada peringkat
- Mechanisms of Cardiac Arrhythmias From Automatici+Dokumen24 halamanMechanisms of Cardiac Arrhythmias From Automatici+Malar MannanBelum ada peringkat
- Science: Quarter 1 - Module 1Dokumen10 halamanScience: Quarter 1 - Module 1RUTH PIANGBelum ada peringkat
- Lim Et Al 2017 PDFDokumen37 halamanLim Et Al 2017 PDFkirshBelum ada peringkat
- 8Dokumen6 halaman8rajanBelum ada peringkat
- B2 Revision PIXLDokumen26 halamanB2 Revision PIXLtunmishetobilawalBelum ada peringkat
- Science (Digestion) Notes/ActivityDokumen4 halamanScience (Digestion) Notes/ActivityHi HelloBelum ada peringkat
- Template POMRDokumen8 halamanTemplate POMRPPDS IPD ULMBelum ada peringkat
- 8 Science NCERT Solutions Chapter 10Dokumen7 halaman8 Science NCERT Solutions Chapter 10Raj Anand100% (1)
- Circulatory System: Heart, Blood Vessels & Their FunctionsDokumen17 halamanCirculatory System: Heart, Blood Vessels & Their FunctionskangaanushkaBelum ada peringkat
- Nervous System - All NotesDokumen6 halamanNervous System - All NotesJBelum ada peringkat
- Form4 NOTES-Nervous SystemDokumen9 halamanForm4 NOTES-Nervous SystemCaroline H DavidBelum ada peringkat
- Worksheet: I) Ii) Iii)Dokumen4 halamanWorksheet: I) Ii) Iii)Jin MingBelum ada peringkat
- L.D..Occlusion in FPDDokumen138 halamanL.D..Occlusion in FPDApurva Deshmukh67% (3)
- Posture and AlignmentDokumen1 halamanPosture and AlignmentNell KeeneBelum ada peringkat
- Lecture 8 - 30.12.2022Dokumen17 halamanLecture 8 - 30.12.2022Adnan Mohammad Adnan HailatBelum ada peringkat
- Refleks ArcsDokumen34 halamanRefleks Arcskiedd_04100% (1)