Diabetic Neuropathy Diagnosis
A doctor reaches a diabetic neuropathy diagnosis based on symptoms, a physical exam, and certain tests. To make a definitive diabetic neuropathy diagnosis, the doctor will do a comprehensive foot exam to assess the skin, circulation, and sensation. Tests used to reach a diabetic neuropathy diagnosis include nerve conduction studies, electromyography (EMG), and ultrasound.
Neuropathies are characterized by a progressive loss of nerve fiber function. A widely accepted definition of diabetic peripheral neuropathy is "the presence of symptoms and/or signs of peripheral nerve dysfunction in people with diabetes after exclusion of other causes."[1] Neuropathies are the most common complication of diabetes mellitus (DM), affecting up to 50% of patients with type 1 and type 2 DM. In type 1 diabetes mellitus, distal polyneuropathy typically becomes symptomatic after many years of chronic prolonged hyperglycemia. Conversely, patients with type 2 diabetes mellitus may present with distal polyneuropathy after only a few years of known poor glycemic control; sometimes, these patients already have neuropathy at the time of diagnosis. (See Clinical Presentation.) Neuropathies severely decrease patients' quality of life (QOL). Furthermore, while the primary symptoms of neuropathy can be highly unpleasant, the secondary complications (eg, falls, foot ulcers, cardiac arrhythmias, and ileus) are even more serious and can lead to fractures, amputations, and even death in patients with DM. Since diabetic neuropathy can manifest with a wide variety of sensory, motor, and autonomic symptoms, a structured list of symptoms can be used to help screen all diabetic patients for possible neuropathy (see History). Physical examination of patients with suspected distal sensory motor or focal (ie, entrapment or noncompressive) neuropathies should include assessments for both peripheral and autonomic neuropathy (see Physical Examination). Multiple consensus panels recommend the inclusion of electrophysiologic testing in the evaluation of diabetic neuropathy. An appropriate array of electrodiagnostic tests includes both nerve conduction testing and needle EMG of the most distal muscles usually affected. (See Workup.) Management of diabetic neuropathy should begin at the initial diagnosis of diabetes. The primary care physician needs to be alert for the development of neuropathyor even its presence at the time of initial diabetes diagnosisbecause failure to diagnose diabetic polyneuropathy can lead to serious consequences, including disability and amputation. In addition, the primary care physician is responsible for educating patients about the acute and chronic complications of diabetes (see Patient Education). Patients with diabetic peripheral neuropathy require more frequent follow-up, with particular attention to foot inspection to reinforce the need for regular self-care. (See Treatment Strategies and Management.) Management of diabetic neuropathy includes 2 approaches: therapies for symptomatic relief and those that may slow the progression of neuropathy. Of all treatments, tight and stable glycemic control is probably the most important for
slowing the progression of neuropathy. Many medications are available for the treatment of diabetic neuropathic pain, although most of them are not specifically approved by the United States Food and Drug Administration for this use. Nonpharmacologic treatment includes rehabilitation, which may comprise physical, occupational, speech, and recreational therapy. (See Medication.)
A review of the anatomy of the peripheral nervous system can facilitate understanding of the classification of diabetic peripheral neuropathy. Peripheral neurons can be categorized broadly as motor, sensory, or autonomic. Motor neurons originate in the central nervous system (CNS) and extend to the anterior horn of the spinal cord. From the anterior horn, they exit the spinal cord (via ventral roots) and combine with other fibers in the brachial or lumbar plexuses and innervate their target organs through peripheral nerves. Sensory neurons originate at the dorsal root ganglia (which lie outside the spinal cord) and follow a similar course with motor neurons. Sensory neurons are subdivided into categories according to the sensory modality they convey (see the Table below). Autonomic neurons consist of sympathetic and parasympathetic types. In the periphery, preganglionic fibers leave the CNS and synapse on postganglionic neurons in the sympathetic chain or in sympathetic ganglia. The smaller fibers are affected first in DM. With continued exposure to hyperglycemia, the larger fibers become affected. Fibers of different size mediate different types of sensation, as shown in the table below. Table. Subdivisions of Sensory Neurons (Open Table in a new window) Fiber Type Size A-alpha (I) A-beta (II) 13-20 micrometers 6-12 micrometers Modality Limb proprioception Myelination Yes
Limb proprioception, vibration, pressure Yes Mechanical sharp pain Yes No
A-delta (III) 1-5 micrometers C (IV)
0.2-1.5 micrometers Thermal pain, mechanical burning pain
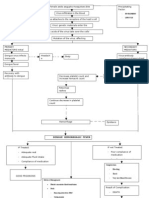
The factors leading to the development of diabetic neuropathy are not understood completely, and multiple hypotheses have been advanced. [2, 3, 4, 5, 6, 7, 8, 9, 10, 11] It is generally accepted to be a multifactorial process. Development of symptoms depends on many factors, such as total hyperglycemic exposure and other risk factors such as elevated lipids, blood pressure, smoking, increased height, and high exposure to other potentially neurotoxic agents such as ethanol. Genetic factors may
also play a role.[12]Important contributing biochemical mechanisms in the development of the more common symmetrical forms of diabetic polyneuropathy likely include the polyol pathway, advanced glycation end products, and oxidative stress. For more information, see Type 2 Diabetes and TCF7L2.
Polyol pathway
Hyperglycemia causes increased levels of intracellular glucose in nerves, leading to saturation of the normal glycolytic pathway. Extra glucose is shunted into the polyol pathway and converted to sorbitol and fructose by the enzymes aldose reductase and sorbitol dehydrogenase.[13] Accumulation of sorbitol and fructose lead to reduced nerve myoinositol, decreased membrane Na+/K+ -ATPase activity, impaired axonal transport, and structural breakdown of nerves, causing abnormal action potential propagation. This is the rationale for the use of aldose reductase inhibitors to improve nerve conduction.[14]
Advanced glycation end products
The nonenzymatic reaction of excess glucose with proteins, nucleotides, and lipids results in advanced glycation end products (ACE) that may have a role in disrupting neuronal integrity and repair mechanisms through interference with nerve cell metabolism and axonal transport.[15]
Oxidative stress
The increased production of free radicals in diabetes may be detrimental via several mechanisms that are not fully understood. These include direct damage to blood vessels leading to nerve ischemia and facilitation of AGE reactions. Despite the incomplete understanding of these processes, use of the antioxidant alpha-lipoic acid may hold promise for improving neuropathic symptoms.[16, 17, 18]
Related contributing factors
Problems that are a consequence of or co-contributors to these disturbed biochemical processes include altered gene expression with altered cellular phenotypes, changes in cell physiology relating to endoskeletal structure or cellular transport, reduction in neurotrophins, and nerve ischemia.[19] Clinical trials of the beststudied neurotrophin, human recombinant nerve growth factor, were disappointing. With future refinements, however, pharmacologic intervention targeting one or more of these mechanisms may prove successful. In the case of focal or asymmetrical diabetic neuropathy syndromes, vascular injury or autoimmunity may play more important roles.[20]
Risk factors that are associated with more severe symptoms include the following[21] :
Poor glycemic control Advanced age Hypertension
Long duration of DM Dyslipidemia Smoking Heavy alcohol intake HLA-DR3/4 phenotype Tall height Development of symptoms depends on many factors, such as total hyperglycemic exposure and other risk factors such as elevated lipids, blood pressure, smoking, increased height, and high exposure to other potentially neurotoxic agents such as ethanol. Genetic factors may also play a role.[12] Peripheral neuropathies have been described in patients with primary DM (types 1 and 2) and in those with secondary diabetes of diverse causes, suggesting a common etiologic mechanism based on chronic hyperglycemia. The contribution of hyperglycemia has received strong support from the Diabetes Control and Complications Trial (DCCT).[22] An association between impaired glucose tolerance and peripheral neuropathy has been construed as further evidence of a dose-dependent effect of hyperglycemia on nerves, although this relationship remains an area of some controversy for type 2 diabetes and prediabetes.[23, 24, 25, 26]
United States statistics
A large American study estimated that 47% of patients with diabetes have some peripheral neuropathy.[27] Neuropathy is estimated to be present in 7.5% of patients at the time of diabetes diagnosis. More than half of cases are distal symmetric polyneuropathy. Focal syndromes such as carpal tunnel syndrome (14-30%),[28, 29, 30] radiculopathies/plexopathies, and cranial neuropathies account for the rest. Solid prevalence data for the latter 2 less-common syndromes is lacking. The wide variability in symmetric diabetic polyneuropathy prevalence data is due to lack of consistent criteria for diagnosis, variable methods of selecting patients for study, and differing assessment techniques. In addition, because many patients with diabetic polyneuropathy are initially asymptomatic, detection is extremely dependent on careful neurologic examination by the primary care clinician. The use of additional diagnostic techniques, such as autonomic or quantitative sensory testing, might result in a higher recorded prevalence.[31, 32]
International statistics
In a cohort of 4400 Belgian patients, Pirart et al found that 7.5% of patients already had neuropathy when diagnosed with diabetes.[33] After 25 years, the number with neuropathy rose to 45%. In the United Kingdom, the prevalence of diabetic neuropathy among the hospital clinic population was noted to be around 29%. [34]
Diabetic neuropathy in racial minorities
No definite racial predilection has been demonstrated for diabetic neuropathy. However, members of minority groups (eg, Hispanics, African Americans) have more secondary complications from diabetic neuropathy, such as lower-extremity
amputations, than whites.[21] They also have more hospitalizations for neuropathic complications.
Sex differences in diabetic neuropathy
DM affects men and women with equal frequency. However, male patients with type 2 diabetes may develop diabetic polyneuropathy earlier than female patients,[35] and neuropathic pain causes more morbidity in females than in males.
Diabetic neuropathy and advancing age
Diabetic neuropathy can occur at any age but is more common with increasing age and severity and duration of diabetes.
Patients with untreated or inadequately treated diabetes have higher morbidity and complication rates related to neuropathy than patients with tightly controlled diabetes. Repetitive trauma to affected areas may cause skin breakdown, progressive ulceration, and infection. Amputations and death may result. Treating diabetic neuropathy is a difficult task for the physician and patient. Most of the medicines mentioned in the Medication section do not lead to complete symptom relief. Clinical trials are under way to help find new ways to treat symptoms and delay disease progression. Mortality is higher in people with cardiovascular autonomic neuropathy (CAN). The overall mortality rate over periods up to 10 years was 27% in patients with DM and CAN detected, compared with a 5% mortality rate in those without evidence of CAN. Morbidity results from foot ulceration and lower-extremity amputation. These 2 complications are the most common causes of hospitalization among people with DM in Western countries. Severe pain, dizziness, diarrhea, and impotence are common symptoms that decrease the QOL of a patient with DM. In patients with diabetic peripheral neuropathy, the prognosis is good, but the patient's QOL is reduced. For more information, go to Diabetic Foot. for more information, go to Diabetic Foot Infections. Controlling diet and nutrition are paramount to improving the secondary complications of diabetes, including neuropathy. Patients with diabetic neuropathy should work with nutritionists or their primary care physicians to develop a realistic diet for lowering blood glucose and minimizing large fluctuations in blood glucose. Patients with diabetic neuropathy should be encouraged to remain as active as possible. However, those with significant sensory loss or autonomic dysfunction should be cautioned about exercising in extreme weather conditions, which may result in injury. For example, patients with extremity numbness may not be aware of frostbite injuries during prolonged cold exposure, or those with abnormal sweating may become easily overheated in hot conditions. In most cases, consultation with the patient's regular physician is reasonable before the initiation of a regular exercise program.
Patients with diabetic neuropathy need to be educated on all aspects of their condition, and they need to know that it is very much affected by poor glycemic control. Prevention of diabetic neuropathy is potentially best achieved by having near-euglycemic control from the onset of DM. Even in patients with symptoms of diabetic neuropathy, controlling blood glucose to euglycemic levels reduces pain significantly. When a person has poor control and becomes euglycemic quickly, pain may be exacerbated (possibly due to an insulin effect), but this pain disappears in a few days. The bottom line for patients is that medications are imperfect. Many result in no pain relief for certain patients. However, glucose control is something that the patient can achieve that may reduce pain. The importance of protection and care of insensitive feet cannot be overemphasized. Patients should be instructed to trim their toenails with great care and to be fastidious about foot hygiene. Any fungal or bacterial infection mandates prompt medical attention. The need for well-fitting shoes should be stressed. Diabetic polyneuropathy is often associated with diabetic retinopathy and nephropathy. Patients with neuropathy should be counseled to seek appropriate eye care and discuss renal care and follow-up with their primary care physicians or endocrinologists. Patient education should begin in the primary care office. The following outline reviews some common questions and answers that can serve as a springboard for discussion.
What is diabetic neuropathy?
Diabetic neuropathy is nerve damage caused by diabetes. In the United States, diabetes is one of the most common causes of nerve damage, also known as peripheral neuropathy. Diabetic neuropathy can affect nerves that supply feeling and movement in the arms and legs. It can also affect the nerves that regulate unconscious vital functions such as heart rate and digestion.
How does diabetic neuropathy occur?
Doctors have been studying this problem for many years, but they do not yet understand exactly how diabetes damages nerves. However, they have observed that good control of blood sugar levels helps prevent diabetic neuropathy and slows its progression, especially in patients with type 1 diabetes.
What are the symptoms?
Symptoms of diabetic neuropathy may include the following:
Numbness or loss of feeling (usually in the feet and legs first, then the hands) Pain Muscle weakness Low blood pressure and dizziness when rising quickly from sitting or lying down Rapid or irregular heartbeats Trouble having an erection Nausea or vomiting Difficulty swallowing
Constipation or diarrhea Pain from diabetic neuropathy may range from minor discomfort or tingling in toes to severe pain. Pain may be sharp or lightning-like, deep and aching, or burning. Extreme sensitivity to the slightest touch can also occur (allodynia).
How can I help prevent diabetic neuropathy?
The following steps may help to prevent or slow the worsening of diabetic neuropathy[36] :
Control diabetes; try to keep blood sugar at a normal level Maintain normal blood pressure Exercise regularly, according to the healthcare provider's recommendation Stop smoking Limit the amount of alcohol intake because excessive alcohol also can cause neuropathy or make it worse Eat a healthy diet and avoid elevated levels of triglycerides in the blood Maintain a healthy weight Keep follow-up appointments with the healthcare provider How is diabetic neuropathy treated? No treatment is currently available to reverse neuropathy. The best approach is to control the diabetes and other risk factors. Muscle weakness is treated with support, such as braces. Physical therapy and regular exercise may help patients maintain the muscle strength they have. Pain medications may help make pain more tolerable. Medications can be used to treat nausea, vomiting, and diarrhea. Men who have trouble having erections because of neuropathy should talk to their healthcare providers. Medications can help a man achieve and maintain an erection, or prosthetic devices can be put in the penis. Preventing injuries such as burns, cuts, or broken bones is especially important, because patients with neuropathy have more complications from simple injuries and may not heal as quickly as healthy individuals.
How can I take care of myself?
Diabetes patients can take the following self-care measures:
Work with primary care physicians and endocrinologists to control glucose levels Examine the skin of feet and lower legs regularly to look for injuries See a healthcare provider promptly for calluses, sores on the skin, or other potential problems so they can be treated properly. Wear good-fitting, comfortable shoes that protect the feet How long will the problem last? Once a person has neuropathy, the symptoms will persist indefinitely, but most people with diabetic neuropathy are able to lead active, fulfilling lives. Keeping blood sugar under good control may stop neuropathy from worsening.
For excellent patient education resources, visit eMedicine's Diabetes Centerand Erectile Dysfunction Center. Also, see eMedicine's patient education articles, Diabetes and Diabetic Foot Care.
Anda mungkin juga menyukai
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- Tvlist IptvDokumen1 halamanTvlist IptvkijokobodroBelum ada peringkat
- MapDokumen37 halamanMapkijokobodroBelum ada peringkat
- BIMx Export LogDokumen1 halamanBIMx Export LogkijokobodroBelum ada peringkat
- Tests Used To Reach A Diabetic Neuropathy DiagnosisDokumen2 halamanTests Used To Reach A Diabetic Neuropathy DiagnosiskijokobodroBelum ada peringkat
- BIMx Export LogDokumen1 halamanBIMx Export LogkijokobodroBelum ada peringkat
- Follow-up of Conservatively Managed Epidural HematomasDokumen7 halamanFollow-up of Conservatively Managed Epidural HematomaskijokobodroBelum ada peringkat
- Complications of Cesarean DeliveryDokumen7 halamanComplications of Cesarean DeliverykijokobodroBelum ada peringkat
- Examining The Safety of Dental Treatment in Pregnant WomenDokumen12 halamanExamining The Safety of Dental Treatment in Pregnant WomenkijokobodroBelum ada peringkat
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Rheumatoid ArthritisDokumen38 halamanRheumatoid ArthritisOlga GoryachevaBelum ada peringkat
- Respiratory System HistologyDokumen32 halamanRespiratory System HistologyMohib HassanBelum ada peringkat
- Understanding Stem Cells: Types, Characteristics and ApplicationsDokumen17 halamanUnderstanding Stem Cells: Types, Characteristics and ApplicationsRebecca Lal MasihBelum ada peringkat
- Dr. Ziad Arandi (Psychiatric MCQS)Dokumen16 halamanDr. Ziad Arandi (Psychiatric MCQS)Firas Anaya100% (1)
- ANENCEPHALYDokumen10 halamanANENCEPHALYSharmaine SimonBelum ada peringkat
- Haralabia BoletiDokumen5 halamanHaralabia BoletiHellenic Pasteur Institute - Athens, GreeceBelum ada peringkat
- B.pharm SyllabusDokumen50 halamanB.pharm SyllabusSunil SharmaBelum ada peringkat
- Application For Job: Date: 17/05/2023Dokumen7 halamanApplication For Job: Date: 17/05/2023Bikila RusiBelum ada peringkat
- Molecular Detection of Extended Spectrum B-Lactamases, MetalloDokumen7 halamanMolecular Detection of Extended Spectrum B-Lactamases, MetalloValentina RondonBelum ada peringkat
- Biol 460 Case StudyDokumen11 halamanBiol 460 Case Studyapi-353888678Belum ada peringkat
- Nephrology MCQSDokumen16 halamanNephrology MCQSThana AlAnsari100% (5)
- Basic Molecular Genetic Mechanisms: (Part 3)Dokumen35 halamanBasic Molecular Genetic Mechanisms: (Part 3)ofirBelum ada peringkat
- ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( - Clinical Trial - (Publication Type) or - Clinical Trials - PubMed - NCBI45Dokumen23 halaman( ( ( ( ( ( ( ( ( ( ( ( ( ( ( - Clinical Trial - (Publication Type) or - Clinical Trials - PubMed - NCBI45Túlio Martins OliveiraBelum ada peringkat
- Proteomics: Technologies and Global MarketsDokumen5 halamanProteomics: Technologies and Global MarketsBCC ResearchBelum ada peringkat
- Psychopathology and Developmental InfluencesDokumen28 halamanPsychopathology and Developmental InfluencesJoy AlexisBelum ada peringkat
- Biology Investigatory ProjectDokumen19 halamanBiology Investigatory ProjectAnsalAshutosh80% (5)
- Biochemistry of The Eye, 2ed. 2003Dokumen331 halamanBiochemistry of The Eye, 2ed. 2003Vuqar100% (3)
- Pathophysio DHF EDITEDDokumen3 halamanPathophysio DHF EDITEDricmichael100% (1)
- Biology 163 Laboratory Prodigiosin Production in Serratia MarcescensDokumen6 halamanBiology 163 Laboratory Prodigiosin Production in Serratia MarcescensRicky Mandala PutraBelum ada peringkat
- Case History TakingDokumen30 halamanCase History Takingvenu238Belum ada peringkat
- Bioactive Natural Products Opportunities and Challenges in MedicinalDokumen695 halamanBioactive Natural Products Opportunities and Challenges in Medicinalney.barbosaBelum ada peringkat
- WJCC 8 1172Dokumen13 halamanWJCC 8 1172johoba5344Belum ada peringkat
- Seizure Disorders: Musupila.M DCM, Adgm, BSC Cs (Unza) 6 November 2019Dokumen26 halamanSeizure Disorders: Musupila.M DCM, Adgm, BSC Cs (Unza) 6 November 2019Emmanuel MukukaBelum ada peringkat
- Spatial Transcriptomics Reveals Distinct and Conserved Tumor Core and Edge Architectures That Predict Survival and Targeted Therapy ResponseDokumen61 halamanSpatial Transcriptomics Reveals Distinct and Conserved Tumor Core and Edge Architectures That Predict Survival and Targeted Therapy Response戴义宾Belum ada peringkat
- Breast Calcifications PDFDokumen8 halamanBreast Calcifications PDFFathan MustafidBelum ada peringkat
- Harr. Cap 114Dokumen7 halamanHarr. Cap 114tkovats.lopes2Belum ada peringkat
- Muscular SystemDokumen20 halamanMuscular SystemAltaf Hussain KhanBelum ada peringkat
- The Nervous System and Reflex Arc (GCSE)Dokumen35 halamanThe Nervous System and Reflex Arc (GCSE)Raja UsamaBelum ada peringkat
- Lessons Learned From The Gene Therapy Trial For OrnithineDokumen7 halamanLessons Learned From The Gene Therapy Trial For OrnithineAfifa ZeeshanBelum ada peringkat
- Books To Follow For CSIR NET ExamDokumen3 halamanBooks To Follow For CSIR NET ExamAbhishek SinghBelum ada peringkat