Anda mungkin juga menyukai
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Septic Arthritis in AdultsDokumen19 halamanSeptic Arthritis in AdultsIvelisse TaverasBelum ada peringkat
- Cephalosporins in Veterinary MedicineDokumen23 halamanCephalosporins in Veterinary MedicineSunil100% (3)
- Treatment of Community-Acquired Pneumonia in Adults Who Require Hospitalization - UpToDateDokumen80 halamanTreatment of Community-Acquired Pneumonia in Adults Who Require Hospitalization - UpToDateTran Thai Huynh NgocBelum ada peringkat
- Historical Overview of The Cephalosporin Spectrum: Four Generations of Structural EvolutionDokumen8 halamanHistorical Overview of The Cephalosporin Spectrum: Four Generations of Structural EvolutionBagus FitraBelum ada peringkat
- Top 10 List of Antibiotic ClassesDokumen10 halamanTop 10 List of Antibiotic ClassesZubair khanBelum ada peringkat
- Medmastery Antimicrobial - Stewardship - HandbookDokumen65 halamanMedmastery Antimicrobial - Stewardship - HandbookHhaBelum ada peringkat
- B-Lactam Ab 2Dokumen34 halamanB-Lactam Ab 2Ph.first SBelum ada peringkat
- DRUG CeftazidimeDokumen1 halamanDRUG Ceftazidimerholiboi0% (1)
- Topic 1 PseudomonashhjjunDokumen8 halamanTopic 1 PseudomonashhjjunRachel Marie M. GaniaBelum ada peringkat
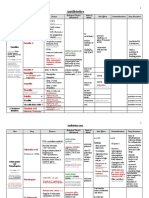
- Antimicrobial Drugs TableDokumen19 halamanAntimicrobial Drugs TableLaylee ClareBelum ada peringkat
- Jurnal BronchopneumoniaDokumen5 halamanJurnal BronchopneumoniaBianti Nur'ainiBelum ada peringkat
- Drug Name Indication Mode of Action Contraindications Side Effects Nursing ConsiderationsDokumen3 halamanDrug Name Indication Mode of Action Contraindications Side Effects Nursing ConsiderationsAlyssa RodriguezBelum ada peringkat
- List of AntibioticsDokumen10 halamanList of AntibioticsPitetLaiBelum ada peringkat
- Febra La Pacientul Imunodeprimat (Romana)Dokumen59 halamanFebra La Pacientul Imunodeprimat (Romana)ialomitaBelum ada peringkat
- CeftazidimeDokumen16 halamanCeftazidimeNakorn BaisriBelum ada peringkat
- Antimicrobial AgentDokumen46 halamanAntimicrobial Agentسامر الرفاعيBelum ada peringkat
- Ivf: Therapeutics: Anti-Pyretics: PenicillinsDokumen6 halamanIvf: Therapeutics: Anti-Pyretics: PenicillinsJenny CiBelum ada peringkat
- Alternative Intravitreal Antibiotics A Systematic.2Dokumen15 halamanAlternative Intravitreal Antibiotics A Systematic.2Daniel MirandaBelum ada peringkat
- Ceftazidime+Avibactum-2gm +0.5gm InjectionDokumen10 halamanCeftazidime+Avibactum-2gm +0.5gm InjectionMd. Abdur RahmanBelum ada peringkat
- Clinical Pharmacokinetics in Burn Patients 1 PDFDokumen8 halamanClinical Pharmacokinetics in Burn Patients 1 PDFClaudio Luis VenturiniBelum ada peringkat
- Antibiotics and Antibacterial Drugs SDokumen67 halamanAntibiotics and Antibacterial Drugs Somar hameed100% (1)
- Nelson's Pediatric Antimicrobial PDFDokumen331 halamanNelson's Pediatric Antimicrobial PDFMADHANKUMAR MANICKAVELBelum ada peringkat
- أدوية الطوارىءDokumen162 halamanأدوية الطوارىءManar22Belum ada peringkat
- Case Study 103Dokumen8 halamanCase Study 103Jonah MaasinBelum ada peringkat
- Continuous and Extended Infusion Beta Lactams PDFDokumen3 halamanContinuous and Extended Infusion Beta Lactams PDFarnaldops333Belum ada peringkat
- Dental RoshetttaDokumen29 halamanDental RoshetttaKORMAX LEAGUEBelum ada peringkat
- Cephalosporins GenerationDokumen7 halamanCephalosporins GenerationSam SmileyBelum ada peringkat
- Antibacerials PharmacolgyDokumen53 halamanAntibacerials PharmacolgyHamid AryanBelum ada peringkat
- 1) Cephalosporins: Generation Common Dosages/Regimens Spectrum of Activity 1 Cephalexin (Keflex) 250-500mg PO q6hDokumen1 halaman1) Cephalosporins: Generation Common Dosages/Regimens Spectrum of Activity 1 Cephalexin (Keflex) 250-500mg PO q6hjoe thomasBelum ada peringkat
- Antibiotic Guideline BIRDEM 2021.pdf Version 1Dokumen92 halamanAntibiotic Guideline BIRDEM 2021.pdf Version 1Imran Khan100% (6)