Anda mungkin juga menyukai
- Breast Augmentation-DR. KAMAL HUSSEIN SALEH-AL EMADI HOSPITALDokumen5 halamanBreast Augmentation-DR. KAMAL HUSSEIN SALEH-AL EMADI HOSPITALDR. KAMAL HUSSEIN SALEH AL HUSSEINYBelum ada peringkat
- Treatments of Lymph Edema of Skin by Liposuction CanulaDokumen6 halamanTreatments of Lymph Edema of Skin by Liposuction CanulaDR. KAMAL HUSSEIN SALEH AL HUSSEINY100% (1)
- BCC of The Nose DR Kamal Hussein Saleh Consultant Cosmetic &plastic Surgery, Al Emadi Hospital-Qatar-DohaDokumen13 halamanBCC of The Nose DR Kamal Hussein Saleh Consultant Cosmetic &plastic Surgery, Al Emadi Hospital-Qatar-DohaDR. KAMAL HUSSEIN SALEH AL HUSSEINYBelum ada peringkat
- Letter A incision periareolar mastopexy with breast implant augmentation-dr. kamal hussein saleh-consultant cosmetic surgeon-al emadi hospital-qatar-doha,زرق ابر البوتوكس,جراحة التجميل,تجميل الانف,تجميل الثدي,تكبير الثدي,تكبير الارداف,مستشفى العمادي,قطر,دبيDokumen5 halamanLetter A incision periareolar mastopexy with breast implant augmentation-dr. kamal hussein saleh-consultant cosmetic surgeon-al emadi hospital-qatar-doha,زرق ابر البوتوكس,جراحة التجميل,تجميل الانف,تجميل الثدي,تكبير الثدي,تكبير الارداف,مستشفى العمادي,قطر,دبيDR. KAMAL HUSSEIN SALEH AL HUSSEINY100% (1)
- Haemangioam DR Kamal Hussain Saleh-Consultant Cosmetic Plastic Surgeon-Al Emadi Hospital-Qatar-DohaDokumen8 halamanHaemangioam DR Kamal Hussain Saleh-Consultant Cosmetic Plastic Surgeon-Al Emadi Hospital-Qatar-DohaDR. KAMAL HUSSEIN SALEH AL HUSSEINY100% (1)
- Haemangioam DR Kamal Hussain Saleh-Consultant Cosmetic Plastic Surgeon-Al Emadi Hospital-Qatar-DohaDokumen8 halamanHaemangioam DR Kamal Hussain Saleh-Consultant Cosmetic Plastic Surgeon-Al Emadi Hospital-Qatar-DohaDR. KAMAL HUSSEIN SALEH AL HUSSEINY100% (1)
- Treatments of Lymph Edema of Skin by Liposuction CanulaDokumen6 halamanTreatments of Lymph Edema of Skin by Liposuction CanulaDR. KAMAL HUSSEIN SALEH AL HUSSEINY100% (1)
- Letter A incision periareolar mastopexy with breast implant augmentation-dr. kamal hussein saleh-consultant cosmetic surgeon-al emadi hospital-qatar-doha,زرق ابر البوتوكس,جراحة التجميل,تجميل الانف,تجميل الثدي,تكبير الثدي,تكبير الارداف,مستشفى العمادي,قطر,دبيDokumen5 halamanLetter A incision periareolar mastopexy with breast implant augmentation-dr. kamal hussein saleh-consultant cosmetic surgeon-al emadi hospital-qatar-doha,زرق ابر البوتوكس,جراحة التجميل,تجميل الانف,تجميل الثدي,تكبير الثدي,تكبير الارداف,مستشفى العمادي,قطر,دبيDR. KAMAL HUSSEIN SALEH AL HUSSEINY100% (1)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5783)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Supreme Court Rules on Retirement Benefits ComputationDokumen5 halamanSupreme Court Rules on Retirement Benefits Computationemman2g.2baccay100% (1)
- A Brief History of The White Nationalist MovementDokumen73 halamanA Brief History of The White Nationalist MovementHugenBelum ada peringkat
- Identification Guide To The Deep-Sea Cartilaginous Fishes of The Indian OceanDokumen80 halamanIdentification Guide To The Deep-Sea Cartilaginous Fishes of The Indian OceancavrisBelum ada peringkat
- HRM Unit 2Dokumen69 halamanHRM Unit 2ranjan_prashant52Belum ada peringkat
- English Course SyllabusDokumen3 halamanEnglish Course Syllabusalea rainBelum ada peringkat
- Exp Mun Feb-15 (Excel)Dokumen7.510 halamanExp Mun Feb-15 (Excel)Vivek DomadiaBelum ada peringkat
- General First Aid QuizDokumen3 halamanGeneral First Aid QuizLucy KiturBelum ada peringkat
- Chapter 1Dokumen30 halamanChapter 1Sneha AgarwalBelum ada peringkat
- Solar Powered Rickshaw PDFDokumen65 halamanSolar Powered Rickshaw PDFPrãvëèñ Hêgådë100% (1)
- Commissioning GuideDokumen78 halamanCommissioning GuideNabilBouabanaBelum ada peringkat
- Jason Payne-James, Ian Wall, Peter Dean-Medicolegal Essentials in Healthcare (2004)Dokumen284 halamanJason Payne-James, Ian Wall, Peter Dean-Medicolegal Essentials in Healthcare (2004)Abdalmonem Albaz100% (1)
- Oilwell Fishing Operations Tools and TechniquesDokumen126 halamanOilwell Fishing Operations Tools and Techniqueskevin100% (2)
- Runner Cs-47 Link Rev-2 27-09-10Dokumen29 halamanRunner Cs-47 Link Rev-2 27-09-10bocko74Belum ada peringkat
- Diagnosis of Dieback Disease of The Nutmeg Tree in Aceh Selatan, IndonesiaDokumen10 halamanDiagnosis of Dieback Disease of The Nutmeg Tree in Aceh Selatan, IndonesiaciptaBelum ada peringkat
- FI - Primeiro Kfir 1975 - 1254 PDFDokumen1 halamanFI - Primeiro Kfir 1975 - 1254 PDFguilhermeBelum ada peringkat
- Mobil Oil v. DiocaresDokumen2 halamanMobil Oil v. DiocaresAntonio Rebosa100% (2)
- Final Literature CircleDokumen10 halamanFinal Literature Circleapi-280793165Belum ada peringkat
- Dhikr or Zikr or Remembrance of AllahDokumen27 halamanDhikr or Zikr or Remembrance of AllahMd. Naim KhanBelum ada peringkat
- Business Beyond Profit Motivation Role of Employees As Decision-Makers in The Business EnterpriseDokumen6 halamanBusiness Beyond Profit Motivation Role of Employees As Decision-Makers in The Business EnterpriseCaladhiel100% (1)
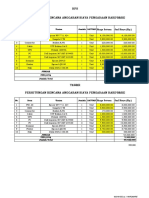
- HPS Perhitungan Rencana Anggaran Biaya Pengadaan Hardware: No. Item Uraian Jumlah SATUANDokumen2 halamanHPS Perhitungan Rencana Anggaran Biaya Pengadaan Hardware: No. Item Uraian Jumlah SATUANYanto AstriBelum ada peringkat
- Block 2 MVA 026Dokumen48 halamanBlock 2 MVA 026abhilash govind mishraBelum ada peringkat
- Perancangan Kota: Jurusan Perencanaan Wilayah Dan Kota Institut Teknologi Nasional Tahun 2021/2022Dokumen27 halamanPerancangan Kota: Jurusan Perencanaan Wilayah Dan Kota Institut Teknologi Nasional Tahun 2021/2022idaBelum ada peringkat
- ZZXCDokumen2 halamanZZXCKrisleen AbrenicaBelum ada peringkat
- All About Linux SignalsDokumen17 halamanAll About Linux SignalsSK_shivamBelum ada peringkat
- Texas COVID-19 Vaccine Distribution PlanDokumen38 halamanTexas COVID-19 Vaccine Distribution PlandmnpoliticsBelum ada peringkat
- E2415 PDFDokumen4 halamanE2415 PDFdannychacon27Belum ada peringkat
- JDDokumen19 halamanJDJuan Carlo CastanedaBelum ada peringkat
- Food and ReligionDokumen8 halamanFood and ReligionAniket ChatterjeeBelum ada peringkat
- Sale of GoodsDokumen41 halamanSale of GoodsKellyBelum ada peringkat
- DPS Chief Michael Magliano DIRECTIVE. Arrests Inside NYS Courthouses April 17, 2019 .Dokumen1 halamanDPS Chief Michael Magliano DIRECTIVE. Arrests Inside NYS Courthouses April 17, 2019 .Desiree YaganBelum ada peringkat