Anda mungkin juga menyukai
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- HRM Chapter 09Dokumen5 halamanHRM Chapter 09Djy DuhamyBelum ada peringkat
- Rules and Principles of Curriculum DevelopmentDokumen4 halamanRules and Principles of Curriculum DevelopmentEvelia Menorca Largo100% (2)
- Youth Version BarOn Emotional Quotient InventoryDokumen4 halamanYouth Version BarOn Emotional Quotient InventorySmriti DhakalBelum ada peringkat
- Topic: Critical Incident Technique: Presenter: Asma ZiaDokumen25 halamanTopic: Critical Incident Technique: Presenter: Asma Ziazia shaikhBelum ada peringkat
- Foster A Growth, Not A Fixed Mindset: Key FindingsDokumen9 halamanFoster A Growth, Not A Fixed Mindset: Key FindingsPablo Barboza JimenezBelum ada peringkat
- Calm Course Outline Hodgson Fall 2014Dokumen2 halamanCalm Course Outline Hodgson Fall 2014api-250760184Belum ada peringkat
- Active Learning MethodDokumen111 halamanActive Learning MethodSudhir VashistBelum ada peringkat
- Credibility Checklist: One Encircled Number For Every Row. Statement Score StatementDokumen2 halamanCredibility Checklist: One Encircled Number For Every Row. Statement Score Statementmauserk98Belum ada peringkat
- Energetic SorceryDokumen26 halamanEnergetic SorceryPete Puza100% (5)
- Alchemy of Emotion (From Bhava To Rasa) (20417)Dokumen13 halamanAlchemy of Emotion (From Bhava To Rasa) (20417)Roxana Cortés100% (1)
- Amazing Race-Eval FormDokumen1 halamanAmazing Race-Eval FormAngela Dianne UbaldoBelum ada peringkat
- Home-School Link: My Learning EssentialsDokumen11 halamanHome-School Link: My Learning EssentialsCV ESBelum ada peringkat
- Assignment No. 1 Principle and Theories of Language Acquisition and Learning - PRELIMDokumen4 halamanAssignment No. 1 Principle and Theories of Language Acquisition and Learning - PRELIMLes SircBelum ada peringkat
- Of Mice and Men' - Cover AnalysisDokumen1 halamanOf Mice and Men' - Cover AnalysisAddie LakeBelum ada peringkat
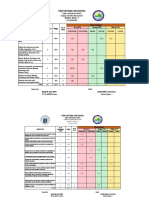
- Mapeh 9 Tos 1ST QuarterDokumen5 halamanMapeh 9 Tos 1ST QuarterKrizha Kate MontausBelum ada peringkat
- MIDTERM-Features of Human Language by HockettDokumen4 halamanMIDTERM-Features of Human Language by HockettBaucas, Rolanda D.100% (1)
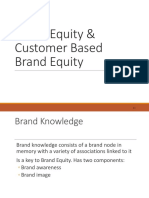
- Brand Equity, CBBE - PPTDokumen26 halamanBrand Equity, CBBE - PPTYashashvi RastogiBelum ada peringkat
- D Epartment of Education: Fourth Quarter Summative Test in English 7Dokumen6 halamanD Epartment of Education: Fourth Quarter Summative Test in English 7Ladylyn Punzalan - SusiBelum ada peringkat
- 5th Lesson Plan Reading A StoryDokumen4 halaman5th Lesson Plan Reading A Storyapi-301142304Belum ada peringkat
- Marxist ApproachDokumen1 halamanMarxist ApproachJoanne Kate BiteroBelum ada peringkat
- RX For Racism: Imperatives For America's Schools - by Gerald J. Pine and Asa G. Hilliard, IIIDokumen10 halamanRX For Racism: Imperatives For America's Schools - by Gerald J. Pine and Asa G. Hilliard, III☥ The Drop Squad Public Library ☥Belum ada peringkat
- Graphic Organizers As Thinking TechnologyDokumen32 halamanGraphic Organizers As Thinking TechnologyGab Ilagan100% (1)
- $R0ACKNFDokumen7 halaman$R0ACKNFjessi NchBelum ada peringkat
- Creative NonfictionDokumen3 halamanCreative NonfictionSheryll Bayya100% (2)
- Stakehokders Appraisal On Work ImmersionDokumen7 halamanStakehokders Appraisal On Work ImmersionVanessa Marbida Bias100% (1)
- GRE High Frequency Words PDFDokumen43 halamanGRE High Frequency Words PDFRohan PrajapatiBelum ada peringkat
- Kirkpatrick's Four Levels of Evaluation: Prepared By: Rachel Marie E. SalongcongDokumen13 halamanKirkpatrick's Four Levels of Evaluation: Prepared By: Rachel Marie E. SalongcongTeacher JanellaBelum ada peringkat
- HG Grade 9 Quarter 1 Module 3 - FrontDokumen3 halamanHG Grade 9 Quarter 1 Module 3 - FrontMary Grace Simbul Mendoza0% (3)
- Retorika Deliberatif Selebgram Dalam Memotivasi Audiens Melalui Media Sosial (Konten  Œlevel Upâ Di Akun Instagram Benakribo)Dokumen8 halamanRetorika Deliberatif Selebgram Dalam Memotivasi Audiens Melalui Media Sosial (Konten  Œlevel Upâ Di Akun Instagram Benakribo)Rebekah KinantiBelum ada peringkat
- 5es OverviewDokumen8 halaman5es OverviewHercules Verdeflor ValenzuelaBelum ada peringkat