Anda mungkin juga menyukai
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (120)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Hand InstrumentsDokumen75 halamanHand Instrumentstarekrabi100% (2)
- Mastering The Chopin Etudes Sample ChaptersDokumen83 halamanMastering The Chopin Etudes Sample Chaptersjoe86% (22)
- Muscles of The Upper Limb 1 PDFDokumen12 halamanMuscles of The Upper Limb 1 PDFDejan MilenkovicBelum ada peringkat
- OITE - 2007 Hand PDFDokumen35 halamanOITE - 2007 Hand PDFICH KhuyBelum ada peringkat
- 1 Magical PassesDokumen7 halaman1 Magical PassesMiloshaaBelum ada peringkat
- DMS (PBL3) Mohamad Arbian Karim FMUI20Dokumen24 halamanDMS (PBL3) Mohamad Arbian Karim FMUI20Mohamad Arbian KarimBelum ada peringkat
- Uts AnatomiDokumen18 halamanUts AnatomiSuratmi UnnesBelum ada peringkat
- Sree Mahaganapathi Tarpana VidhiDokumen19 halamanSree Mahaganapathi Tarpana Vidhim.s.subramania sharmaBelum ada peringkat
- Cuestionario Kamath y StothardDokumen4 halamanCuestionario Kamath y StothardPasha Camacho100% (1)
- U1D800Dokumen13 halamanU1D800ElsaBelum ada peringkat
- A New Hand Exoskeleton Device For Rehabilitation Using A Three-Layered Sliding Spring Mechanism PDFDokumen6 halamanA New Hand Exoskeleton Device For Rehabilitation Using A Three-Layered Sliding Spring Mechanism PDFGIenlemenBelum ada peringkat
- Pediatric Tuina TherapyDokumen79 halamanPediatric Tuina TherapyHu Xiao100% (1)
- Lesson PlansDokumen15 halamanLesson Plansapi-455930823Belum ada peringkat
- EPL - EXERCISE OF PRACTICAL LIFE - Supriya JainDokumen32 halamanEPL - EXERCISE OF PRACTICAL LIFE - Supriya JainṦafia Naz100% (1)
- Muscles MastersheetDokumen37 halamanMuscles MastersheetmargaritaBelum ada peringkat
- Wajah: Dan PengunyohDokumen8 halamanWajah: Dan PengunyohRetno Noor FebbyBelum ada peringkat
- 2008 Article 9145-2 PDFDokumen7 halaman2008 Article 9145-2 PDFDeborah González GarcíaBelum ada peringkat
- Anatomy of Wrist and HandDokumen27 halamanAnatomy of Wrist and HandMaria Russel Vitualla100% (2)
- Muscles of The ScapulaDokumen6 halamanMuscles of The ScapulaAndika Anjani AgustinBelum ada peringkat
- Massage 101Dokumen33 halamanMassage 101Vladislav KotovBelum ada peringkat
- Upper Limb Lecture 1Dokumen45 halamanUpper Limb Lecture 1fdjkvfjvBelum ada peringkat
- Anatomy of Forearm and WristDokumen47 halamanAnatomy of Forearm and WristYnolde LeysBelum ada peringkat
- 1.01 Reaction TimeDokumen1 halaman1.01 Reaction TimeAnshu MovvaBelum ada peringkat
- CASE4Dokumen9 halamanCASE4Jan Marc SantosBelum ada peringkat
- Komatsu Wheeled Excavator Pw160 8 Shop Manual Venbm61000 2012Dokumen22 halamanKomatsu Wheeled Excavator Pw160 8 Shop Manual Venbm61000 2012ryanchambers010800rsc100% (117)
- Group Personal Accident Product SummaryDokumen11 halamanGroup Personal Accident Product SummarySS CheeBelum ada peringkat
- 55 Pain in The Arm and HandsDokumen22 halaman55 Pain in The Arm and Handsprofarmah6150Belum ada peringkat
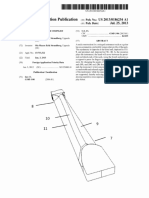
- Trapezoidal Neck Strandberg US20130186254A1Dokumen10 halamanTrapezoidal Neck Strandberg US20130186254A1Percy Stanbury Malaga100% (1)
- Kevin Kunz and Barbara Kunz - Hand Reflexology WorkbookDokumen132 halamanKevin Kunz and Barbara Kunz - Hand Reflexology WorkbookPedro C.100% (3)
- Salman-Outcome of Tendon Transfer Surgery For Radial NerveDokumen4 halamanSalman-Outcome of Tendon Transfer Surgery For Radial Nervearief setyo nugrohoBelum ada peringkat