Anda mungkin juga menyukai
- GO S For Tamilnadu DoctorsDokumen160 halamanGO S For Tamilnadu DoctorsSuresh KumarBelum ada peringkat
- Spinal Anesthesia For Caeserian Section: Comparison of 5.0% Lignocaine and 0.5% BupivacaineDokumen4 halamanSpinal Anesthesia For Caeserian Section: Comparison of 5.0% Lignocaine and 0.5% BupivacaineSuresh KumarBelum ada peringkat
- Local Anaesthetic AgentsDokumen21 halamanLocal Anaesthetic AgentsSuresh KumarBelum ada peringkat
- Anaesthesia Care Beyond Operating Rooms: Newer Opportunities & Challenges.Dokumen8 halamanAnaesthesia Care Beyond Operating Rooms: Newer Opportunities & Challenges.Suresh Kumar100% (1)
- Perioperative Management of A Patient With Left Ventricular FailureDokumen6 halamanPerioperative Management of A Patient With Left Ventricular FailureSuresh KumarBelum ada peringkat
- Ventilator Associated Pneumonia (Vap)Dokumen11 halamanVentilator Associated Pneumonia (Vap)Suresh KumarBelum ada peringkat
- Anaesthetic Management of Blunt Chest TraumaDokumen11 halamanAnaesthetic Management of Blunt Chest TraumaSuresh KumarBelum ada peringkat
- Controversial Issues in NeuroanaesthesiaDokumen12 halamanControversial Issues in NeuroanaesthesiaSuresh KumarBelum ada peringkat
- Medico-Legal Issues in AnaesthesiaDokumen2 halamanMedico-Legal Issues in AnaesthesiaSuresh KumarBelum ada peringkat
- Cerebral Protection What Is New ?Dokumen11 halamanCerebral Protection What Is New ?Suresh Kumar100% (1)
- Day Care AnesthesiaDokumen4 halamanDay Care AnesthesiaSuresh KumarBelum ada peringkat
- Alleviating Cancer PainDokumen9 halamanAlleviating Cancer PainSuresh KumarBelum ada peringkat
- Muscle Relaxants in Current PracticeDokumen6 halamanMuscle Relaxants in Current PracticeSuresh KumarBelum ada peringkat
- Role of The Anaesthesiologists in The Management of BurnsDokumen12 halamanRole of The Anaesthesiologists in The Management of BurnsSuresh KumarBelum ada peringkat
- Anaesthesia in The Gastrointestinal Endoscopy SuiteDokumen3 halamanAnaesthesia in The Gastrointestinal Endoscopy SuiteSuresh KumarBelum ada peringkat
- Analysis of Arterial Blood GasesDokumen17 halamanAnalysis of Arterial Blood GasesSuresh KumarBelum ada peringkat
- Surgical Patients at Risk For Renal FailureDokumen35 halamanSurgical Patients at Risk For Renal FailureSuresh KumarBelum ada peringkat
- Anesthesia For Fetal SurgeryDokumen8 halamanAnesthesia For Fetal SurgerySuresh KumarBelum ada peringkat
- Anaesthesia For Bleeding TonsilDokumen6 halamanAnaesthesia For Bleeding TonsilSave MedicalEducation Save HealthCareBelum ada peringkat
- Anaesthetic Management of Bleeding Obstetric PatientDokumen10 halamanAnaesthetic Management of Bleeding Obstetric PatientSuresh KumarBelum ada peringkat
- Pre-Operative Cardio-Pulmonary Exercise Testing (Cpet)Dokumen14 halamanPre-Operative Cardio-Pulmonary Exercise Testing (Cpet)Suresh KumarBelum ada peringkat
- Labour Analgesia - Recent ConceptsDokumen18 halamanLabour Analgesia - Recent ConceptsSuresh KumarBelum ada peringkat
- Depth of Anesthesia & MonitoringDokumen2 halamanDepth of Anesthesia & MonitoringSuresh KumarBelum ada peringkat
- Anaesthetic Management of Ihd Patients For Non Cardiac SurgeryDokumen18 halamanAnaesthetic Management of Ihd Patients For Non Cardiac SurgerySuresh KumarBelum ada peringkat
- Preoperative Anaesthetic Risk Assessment and Risk Reduction Before SurgeryDokumen17 halamanPreoperative Anaesthetic Risk Assessment and Risk Reduction Before SurgerySuresh KumarBelum ada peringkat
- Anaesthesia Breathing SystemsDokumen15 halamanAnaesthesia Breathing SystemsSuresh KumarBelum ada peringkat
- Anaesthetic Management of Patients With Pacemakers and Implantable Cardioverter Defibrillator.Dokumen16 halamanAnaesthetic Management of Patients With Pacemakers and Implantable Cardioverter Defibrillator.Suresh KumarBelum ada peringkat
- Basic Physics Applied To AnaesthesiologyDokumen10 halamanBasic Physics Applied To AnaesthesiologySuresh KumarBelum ada peringkat
- Fluid Resuscitation in TraumaDokumen17 halamanFluid Resuscitation in TraumaSuresh Kumar100% (1)
- Pulmonary Function Test in Pre Anaesthetic EvaluationDokumen10 halamanPulmonary Function Test in Pre Anaesthetic EvaluationSuresh KumarBelum ada peringkat
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5784)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Laws of MotionDokumen64 halamanLaws of MotionArnel A. JulatonBelum ada peringkat
- EASA TCDS E.007 (IM) General Electric CF6 80E1 Series Engines 02 25102011Dokumen9 halamanEASA TCDS E.007 (IM) General Electric CF6 80E1 Series Engines 02 25102011Graham WaterfieldBelum ada peringkat
- IntroductionDokumen34 halamanIntroductionmarranBelum ada peringkat
- PCSE_WorkbookDokumen70 halamanPCSE_WorkbookWilliam Ribeiro da SilvaBelum ada peringkat
- Embryo If Embryonic Period PDFDokumen12 halamanEmbryo If Embryonic Period PDFRyna Miguel MasaBelum ada peringkat
- Give Five Examples Each of Nature Having Reflection Symmetry and Radial Symmetry Reflection Symmetry Radial Symmetry Butterfly StarfishDokumen12 halamanGive Five Examples Each of Nature Having Reflection Symmetry and Radial Symmetry Reflection Symmetry Radial Symmetry Butterfly StarfishANNA MARY GINTOROBelum ada peringkat
- All Associates Warning Against ChangesDokumen67 halamanAll Associates Warning Against Changesramesh0% (1)
- Computer Portfolio (Aashi Singh)Dokumen18 halamanComputer Portfolio (Aashi Singh)aashisingh9315Belum ada peringkat
- Creatures Since Possible Tanks Regarding Dengue Transmission A Planned Out ReviewjnspeDokumen1 halamanCreatures Since Possible Tanks Regarding Dengue Transmission A Planned Out Reviewjnspeclientsunday82Belum ada peringkat
- TLE8 Q4 Week 8 As Food ProcessingDokumen4 halamanTLE8 Q4 Week 8 As Food ProcessingROSELLE CASELABelum ada peringkat
- PW CDokumen4 halamanPW CAnonymous DduElf20OBelum ada peringkat
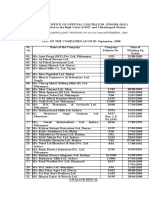
- Statement of Compulsory Winding Up As On 30 SEPTEMBER, 2008Dokumen4 halamanStatement of Compulsory Winding Up As On 30 SEPTEMBER, 2008abchavhan20Belum ada peringkat
- (Bio) Chemistry of Bacterial Leaching-Direct vs. Indirect BioleachingDokumen17 halaman(Bio) Chemistry of Bacterial Leaching-Direct vs. Indirect BioleachingKatherine Natalia Pino Arredondo100% (1)
- Mechanics of Deformable BodiesDokumen21 halamanMechanics of Deformable BodiesVarun. hrBelum ada peringkat
- For Coin & Blood (2nd Edition) - SicknessDokumen16 halamanFor Coin & Blood (2nd Edition) - SicknessMyriam Poveda50% (2)
- Control SystemsDokumen269 halamanControl SystemsAntonis SiderisBelum ada peringkat
- C Exam13Dokumen4 halamanC Exam13gauravsoni1991Belum ada peringkat
- Domingo V People (Estafa)Dokumen16 halamanDomingo V People (Estafa)Kim EscosiaBelum ada peringkat
- Individual Sports Prelim ExamDokumen13 halamanIndividual Sports Prelim ExamTommy MarcelinoBelum ada peringkat
- Installation Instruction XALM IndoorDokumen37 halamanInstallation Instruction XALM IndoorVanek505Belum ada peringkat
- Emerson Park Master Plan 2015 DraftDokumen93 halamanEmerson Park Master Plan 2015 DraftRyan DeffenbaughBelum ada peringkat
- GIS Arrester PDFDokumen0 halamanGIS Arrester PDFMrC03Belum ada peringkat
- Product CycleDokumen2 halamanProduct CycleoldinaBelum ada peringkat
- Board 2Dokumen1 halamanBoard 2kristine_nilsen_2Belum ada peringkat
- NGPDU For BS SelectDokumen14 halamanNGPDU For BS SelectMario RamosBelum ada peringkat
- Liber Chao (Final - Eng)Dokumen27 halamanLiber Chao (Final - Eng)solgrae8409100% (2)
- MMW FinalsDokumen4 halamanMMW FinalsAsh LiwanagBelum ada peringkat
- ExpDokumen425 halamanExpVinay KamatBelum ada peringkat
- Class Ix - Break-Up SyllabusDokumen3 halamanClass Ix - Break-Up Syllabus9C Aarib IqbalBelum ada peringkat
- 10 Slides For A Perfect Startup Pitch DeckDokumen6 halaman10 Slides For A Perfect Startup Pitch DeckZakky AzhariBelum ada peringkat