Anda mungkin juga menyukai
- Ischemic StrokeDokumen49 halamanIschemic StrokeMirna Ayu Permata SariBelum ada peringkat
- Stroke PathophysiologyDokumen3 halamanStroke PathophysiologyMaureen Balagtas89% (9)
- Stroke PathophysiologyDokumen3 halamanStroke PathophysiologyMaureen EricaBelum ada peringkat
- Hemorrhagic StrokeDokumen30 halamanHemorrhagic StrokeAstrina SupandyBelum ada peringkat
- Essential Guide to Diagnosing and Treating Ischemic StrokeDokumen21 halamanEssential Guide to Diagnosing and Treating Ischemic Strokekuchaibaru90Belum ada peringkat
- Hemorrhagic StrokeDokumen12 halamanHemorrhagic StrokeManggara Surya DharmaBelum ada peringkat
- Hemorrhagic StrokeDokumen27 halamanHemorrhagic StrokeMuhammad FarhanBelum ada peringkat
- Pathophysiology of Spinal Cord Injury ExplainedDokumen5 halamanPathophysiology of Spinal Cord Injury ExplainedUmar FarooqBelum ada peringkat
- Bachelor of Nursing Science With HonoursDokumen17 halamanBachelor of Nursing Science With HonoursMaryam HasanahBelum ada peringkat
- Transient Ischemic AttackDokumen69 halamanTransient Ischemic AttackAllen Rolan Losaria100% (3)
- Hemorrhagic Stroke: Darpen Subhashbhai Mori Group 2, MD 3BDokumen13 halamanHemorrhagic Stroke: Darpen Subhashbhai Mori Group 2, MD 3BDarpen MoriBelum ada peringkat
- CASE-STUDY HEMORRHAGIC-STROKE FinalDokumen102 halamanCASE-STUDY HEMORRHAGIC-STROKE FinalAngela Quiñones67% (3)
- Spinal Cord InjuryDokumen37 halamanSpinal Cord InjuryArfian Deny PBelum ada peringkat
- Group 4 - Hemorrhagic StrokeDokumen60 halamanGroup 4 - Hemorrhagic StrokeKitz T AnasarioBelum ada peringkat
- Cerebrovascular AccidentDokumen8 halamanCerebrovascular Accidentplethoraldork100% (10)
- Head Injury Causes and TreatmentDokumen47 halamanHead Injury Causes and TreatmentnikowareBelum ada peringkat
- Middle Cerebral Artery (MCA) Infarcts: Symptoms and LocationsDokumen4 halamanMiddle Cerebral Artery (MCA) Infarcts: Symptoms and Locationskat9210Belum ada peringkat
- Case Study CVDDokumen49 halamanCase Study CVDJasmine Yen Urguelles GaringanBelum ada peringkat
- Pathophysiology of StrokeDokumen11 halamanPathophysiology of StrokeAgronaSlaughterBelum ada peringkat
- Craniotomy: Brain Tumors Aneurysms AvmsDokumen5 halamanCraniotomy: Brain Tumors Aneurysms AvmsMichael Cody SoBelum ada peringkat
- Pathophysiology TBIDokumen1 halamanPathophysiology TBIChester ManaloBelum ada peringkat
- Pathophysiology and Risk Factors of Stroke (CVADokumen7 halamanPathophysiology and Risk Factors of Stroke (CVACHANDAN RAIBelum ada peringkat
- EncephalitisDokumen20 halamanEncephalitisBenita Putri MDBelum ada peringkat
- Subarachnoid HemorrhageDokumen2 halamanSubarachnoid HemorrhageJethro Bacayo Zamora100% (1)
- Cerebellar DisordersDokumen12 halamanCerebellar DisordersAnn SamBelum ada peringkat
- Subdural HematomaDokumen20 halamanSubdural HematomaArief Zamir100% (1)
- Pathophysiology of Acute Ischemic StrokeDokumen12 halamanPathophysiology of Acute Ischemic Strokeidno1008100% (2)
- Guillain Barre Syndrome (GBS) ImanDokumen26 halamanGuillain Barre Syndrome (GBS) ImanTowardsLight100% (5)
- Case-Study Hemorrhagic-Stroke FinalDokumen102 halamanCase-Study Hemorrhagic-Stroke FinalAngela QuiñonesBelum ada peringkat
- Cerebrovascular Accident I. General Medical Background A. DefinitionDokumen11 halamanCerebrovascular Accident I. General Medical Background A. Definitionner100% (1)
- INTRODUCTION A Cerebrovascular Accident (CVA), An Ischemic Stroke or "BrainDokumen30 halamanINTRODUCTION A Cerebrovascular Accident (CVA), An Ischemic Stroke or "BrainCherie May100% (5)
- Case Presentation of Hemorrhagic Stroke (Subarachnoid Hemorrhage)Dokumen69 halamanCase Presentation of Hemorrhagic Stroke (Subarachnoid Hemorrhage)verna88% (24)
- Amyotrophic Lateral SclerosisDokumen13 halamanAmyotrophic Lateral SclerosisBryan Andrew GonzalesBelum ada peringkat
- Spinal Cord InjuryDokumen64 halamanSpinal Cord InjuryKrishan_Bansal_2247Belum ada peringkat
- Stroke PathophysiologyDokumen2 halamanStroke PathophysiologyJaessa Feliciano100% (2)
- Hip FracturesDokumen7 halamanHip FracturesDinly JoyBelum ada peringkat
- Transient Ischemic Attack: A Case StudyDokumen44 halamanTransient Ischemic Attack: A Case Studytinay100% (8)
- Congestive Heart FailureDokumen15 halamanCongestive Heart FailureChiraz Mwangi100% (1)
- CVADokumen11 halamanCVACla100% (4)
- Spinal Cord InjuryDokumen9 halamanSpinal Cord InjurytasneemBelum ada peringkat
- Spinal Cord InjuryDokumen16 halamanSpinal Cord Injuryjohnlester_jlf100% (2)
- Multiple SclerosisDokumen43 halamanMultiple SclerosisProdan SimonaBelum ada peringkat
- Traumatic Brain InjuryDokumen32 halamanTraumatic Brain InjuryNayan Maharjan100% (1)
- Cerebellar InfarctionDokumen23 halamanCerebellar InfarctionShane LuyBelum ada peringkat
- Handout Orthopedic Nursing Spinal Cord InjuryDokumen8 halamanHandout Orthopedic Nursing Spinal Cord InjuryPaul Christian P. Santos, RNBelum ada peringkat
- Case Study On Stroke PatientDokumen2 halamanCase Study On Stroke PatientsparrowcrowBelum ada peringkat
- Types of Head Injuries and Their SymptomsDokumen5 halamanTypes of Head Injuries and Their SymptomsRhomz Zubieta RamirezBelum ada peringkat
- Understanding Stroke: Causes, Types and Risk FactorsDokumen57 halamanUnderstanding Stroke: Causes, Types and Risk FactorsAishwarya ShahBelum ada peringkat
- Case Presentation About Spinal Shock SyndromeDokumen56 halamanCase Presentation About Spinal Shock SyndromeAstral_edge010100% (1)
- CVA Case StudyDokumen9 halamanCVA Case Studypylzanne100% (1)
- Pathophysiology of TBI 97Dokumen51 halamanPathophysiology of TBI 97rajan kumarBelum ada peringkat
- Subarachnoid HemorrhageDokumen74 halamanSubarachnoid HemorrhageDr. Kishore Kumar Ubrangala100% (1)
- Case Study StrokeDokumen40 halamanCase Study Strokeymonn100% (1)
- Cerebral AneurysmDokumen24 halamanCerebral Aneurysmcaptain_rafeBelum ada peringkat
- Pathophysiology HeadinjuryDokumen1 halamanPathophysiology HeadinjuryK.b. Dequiña100% (1)
- General Pathophysiology: Predisposing Factors: Precipitating FactorsDokumen2 halamanGeneral Pathophysiology: Predisposing Factors: Precipitating FactorsIrish Nicole DCBelum ada peringkat
- Types and Causes of Hemorrhagic StrokesDokumen7 halamanTypes and Causes of Hemorrhagic StrokesRavinr9Belum ada peringkat
- Cerebral HemorrhageDokumen2 halamanCerebral HemorrhageGian TejadaBelum ada peringkat
- Subarachnoid Hemorrhage - Stroke (CVA) - Merck Manual Home Edition2Dokumen8 halamanSubarachnoid Hemorrhage - Stroke (CVA) - Merck Manual Home Edition2Noval LiadyBelum ada peringkat
- By. ScribdDokumen3 halamanBy. Scribdchreazy__021906Belum ada peringkat
- Breakdown BHP LabDokumen39 halamanBreakdown BHP LabNdan RahmaBelum ada peringkat
- Cara Menyusui Yang BenarDokumen1 halamanCara Menyusui Yang BenarNdan RahmaBelum ada peringkat
- TGL PULANG Diminta Dr. HarryDokumen1 halamanTGL PULANG Diminta Dr. HarryNdan RahmaBelum ada peringkat
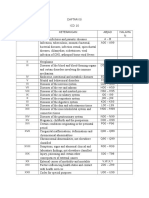
- Icd 10Dokumen2 halamanIcd 10Ndan RahmaBelum ada peringkat
- Icd 10 EditDokumen96 halamanIcd 10 EditNdan RahmaBelum ada peringkat
- TGL PULANG Diminta Dr. HarryDokumen1 halamanTGL PULANG Diminta Dr. HarryNdan RahmaBelum ada peringkat
- Post Partum Hemorhage Dan Management in Clinical Emergency - Sragen 2014-1Dokumen59 halamanPost Partum Hemorhage Dan Management in Clinical Emergency - Sragen 2014-1Ndan Rahma100% (2)
- List Barang LabDokumen9 halamanList Barang LabNdan RahmaBelum ada peringkat
- Icd 9 CMDokumen1 halamanIcd 9 CMNdan RahmaBelum ada peringkat
- List Barang LabDokumen9 halamanList Barang LabNdan RahmaBelum ada peringkat
- Stroke Hemoragik: Gejala, Diagnosis, dan Pengobatan UtamaDokumen20 halamanStroke Hemoragik: Gejala, Diagnosis, dan Pengobatan UtamaTriana AmaliaBelum ada peringkat
- Prokaryotic Cells: Eukaryotes Vs Prokaryotes: What's The Difference?Dokumen8 halamanProkaryotic Cells: Eukaryotes Vs Prokaryotes: What's The Difference?Anggun Teh PamegetBelum ada peringkat
- Assessment of Fluid and ElectrolyteDokumen15 halamanAssessment of Fluid and ElectrolyteDip Ayan MBelum ada peringkat
- Aqa Byb1 W QP Jun07Dokumen12 halamanAqa Byb1 W QP Jun07李超然Belum ada peringkat
- Throwing RehabDokumen16 halamanThrowing RehabSean GlynnBelum ada peringkat
- Drug StudyDokumen14 halamanDrug StudyTin BernardezBelum ada peringkat
- MicronutrientsDokumen21 halamanMicronutrientsJohn Paolo OcampoBelum ada peringkat
- Snakes in India - Tradition and The Truth PDFDokumen5 halamanSnakes in India - Tradition and The Truth PDFhoticeforuBelum ada peringkat
- Binocular Anomalies - GriffinDokumen595 halamanBinocular Anomalies - GriffinAdolph Grey75% (4)
- Big Can Be Beautiful, TIVA in The ObeseDokumen7 halamanBig Can Be Beautiful, TIVA in The ObeseHernán GiménezBelum ada peringkat
- 12 White Blood Cell Counting Techniques in BirdsDokumen5 halaman12 White Blood Cell Counting Techniques in BirdsPablo LópezBelum ada peringkat
- Pregnant woman with painful swollen legDokumen12 halamanPregnant woman with painful swollen legjimmojonesBelum ada peringkat
- Chapter 31 - Assessment and Management of Patients With Vascular DisordersDokumen7 halamanChapter 31 - Assessment and Management of Patients With Vascular DisordersMichael Boado100% (1)
- BIO01 CO1 PPT - An Overview of The CellDokumen60 halamanBIO01 CO1 PPT - An Overview of The CellCHRISTIAN MATTHEW DELA CRUZBelum ada peringkat
- LP UapDokumen18 halamanLP UapHat MutisalBelum ada peringkat
- Dental Appliances For Snoring and Obstructive Sleep Apnoea - Construction Aspects For General Dental PractitionersDokumen9 halamanDental Appliances For Snoring and Obstructive Sleep Apnoea - Construction Aspects For General Dental Practitionersdocx1975100% (1)
- Brewing Technology (2017)Dokumen190 halamanBrewing Technology (2017)Јован АдамовBelum ada peringkat
- Dr. Sak Indriyani, Spa, Mkes: Department of Child Health Rsu MataramDokumen48 halamanDr. Sak Indriyani, Spa, Mkes: Department of Child Health Rsu MataramMuhammad Bilal Bin AmirBelum ada peringkat
- 3B Arm Model - M11Dokumen28 halaman3B Arm Model - M11rswongym449Belum ada peringkat
- Proteinuria and Chronic Kidney DiseaseDokumen34 halamanProteinuria and Chronic Kidney DiseaseВалерий ГаврилуцаBelum ada peringkat
- Module 4-The Cell's Life CycleDokumen5 halamanModule 4-The Cell's Life CycleGoogle BackupBelum ada peringkat
- Simple Non-Ruminants: Principles of Animal Nutrition Dr. Cristine W. MaramagDokumen30 halamanSimple Non-Ruminants: Principles of Animal Nutrition Dr. Cristine W. MaramagMc Kjell Dagman RaveloBelum ada peringkat
- Principles & Practice of First AidDokumen298 halamanPrinciples & Practice of First AidJoshua100% (2)
- Sarns Modular Perfusion System 8000: A Flexible, Dependable, and Cost-Efficient Modular Blood Pumping SystemDokumen4 halamanSarns Modular Perfusion System 8000: A Flexible, Dependable, and Cost-Efficient Modular Blood Pumping SystemAdvancemicronics MedicalsystemsBelum ada peringkat
- COPD and Lower Respiratory Infection GuideDokumen4 halamanCOPD and Lower Respiratory Infection GuideIch RamBelum ada peringkat
- Neuropathic Painn PDFDokumen20 halamanNeuropathic Painn PDFkaktusBelum ada peringkat
- Receptors IntroductionDokumen53 halamanReceptors IntroductionSunilBelum ada peringkat
- Amphibian Graphs?Dokumen9 halamanAmphibian Graphs?Anshumaan PatraBelum ada peringkat
- Who Needs Bypass SurgeryDokumen70 halamanWho Needs Bypass SurgerymikikiBelum ada peringkat
- Surgical Resection of Cancer of The Buccal MucosaDokumen21 halamanSurgical Resection of Cancer of The Buccal MucosapradeepBelum ada peringkat
- Armstrong, Mechele - Blood Lines 05 - Bitter LoveDokumen126 halamanArmstrong, Mechele - Blood Lines 05 - Bitter LoveMenahil BasitBelum ada peringkat