Anda mungkin juga menyukai
- Antibiotic Summary - DraftDokumen10 halamanAntibiotic Summary - DraftStrept Pneumonia100% (1)
- Classification of AntibioticsDokumen4 halamanClassification of AntibioticsNico AvellanaBelum ada peringkat
- Antibiotics.: Prepared by L.Mbise OCTOBER 2012Dokumen40 halamanAntibiotics.: Prepared by L.Mbise OCTOBER 2012Moses MberwaBelum ada peringkat
- Pharmacology Section on Antibiotics, Antivirals and AntifungalsDokumen5 halamanPharmacology Section on Antibiotics, Antivirals and AntifungalsPathalee ThalpavilaBelum ada peringkat
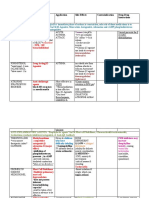
- Drug Name Mechanism Application Side Effects Contraindication Drug-Drug InteractionsDokumen3 halamanDrug Name Mechanism Application Side Effects Contraindication Drug-Drug Interactionsazhar hussinBelum ada peringkat
- Quinolones, Folic Acid Antagonist and Urinary Tract Antitb and LeprosyDokumen124 halamanQuinolones, Folic Acid Antagonist and Urinary Tract Antitb and LeprosyrenBelum ada peringkat
- Anti Emetic DrugsDokumen3 halamanAnti Emetic DrugsFaria Islam JuhiBelum ada peringkat
- Antibiotic GuideDokumen6 halamanAntibiotic GuideAnnTran100% (1)
- Mu 002Dokumen10 halamanMu 002chandanBelum ada peringkat
- Drug Outline: Autonomic Nervous System Drug Class Drug OtherDokumen4 halamanDrug Outline: Autonomic Nervous System Drug Class Drug OtherCess Lagera YbanezBelum ada peringkat
- Manteux TestDokumen25 halamanManteux TestEvaNatashaBelum ada peringkat
- Augmenten (Amoxicillin Clavulan)Dokumen2 halamanAugmenten (Amoxicillin Clavulan)Adrianne BazoBelum ada peringkat
- Anti-Retro Viral DrugsDokumen33 halamanAnti-Retro Viral Drugsapi-306036754Belum ada peringkat
- Antidiarrheal DrugsDokumen4 halamanAntidiarrheal DrugsNadhirah ZulkifliBelum ada peringkat
- Top 10 Drug InteractionsDokumen4 halamanTop 10 Drug InteractionsLeyla MajundaBelum ada peringkat
- Aminogycoside AntibioticsDokumen31 halamanAminogycoside AntibioticsNurul Febrina100% (2)
- Non-Steroidal Anti Inflammatory Drugs (NSAIDS)Dokumen5 halamanNon-Steroidal Anti Inflammatory Drugs (NSAIDS)Pardhasaradhi PantaBelum ada peringkat
- TizanidineDokumen2 halamanTizanidinebhawanisrBelum ada peringkat
- Pharmacology of The GITDokumen31 halamanPharmacology of The GITmarviecute22Belum ada peringkat
- Protein-Calorie Malnutrition Legal RiskDokumen6 halamanProtein-Calorie Malnutrition Legal RiskfirdakusumaputriBelum ada peringkat
- Anti-Infectives and AntibioticsDokumen38 halamanAnti-Infectives and AntibioticsKarel Lu0% (1)
- DrugsDokumen20 halamanDrugsLee Won100% (1)
- SAQ Short Form 2006Dokumen1 halamanSAQ Short Form 2006Hanan DaghashBelum ada peringkat
- Nursing Theory: Asthma (Presentation)Dokumen13 halamanNursing Theory: Asthma (Presentation)vinda astri permatasari100% (1)
- ClindamycinDokumen3 halamanClindamycinShaira TanBelum ada peringkat
- Anti-Infective Pharmacology ReviewerDokumen5 halamanAnti-Infective Pharmacology ReviewerArianne Pearl PrimeroBelum ada peringkat
- Chemotherapy NDokumen28 halamanChemotherapy NFaisal MehboobBelum ada peringkat
- Drug Card Solu-MEDROLDokumen2 halamanDrug Card Solu-MEDROLBenBelum ada peringkat
- Generic Name Brand Names Common Uses Possible Side Effects Mechanism of ActionDokumen13 halamanGeneric Name Brand Names Common Uses Possible Side Effects Mechanism of Actionangel3424Belum ada peringkat
- Antibiotics 9Dokumen11 halamanAntibiotics 9Beth Morales100% (1)
- Animal Bites Approach GuideDokumen39 halamanAnimal Bites Approach GuideNetii FarhatiBelum ada peringkat
- Asthma Inhaler Device Techiques ChecklistDokumen2 halamanAsthma Inhaler Device Techiques Checklistdaniel ragonjanBelum ada peringkat
- Cholinergic Drugs - TablesDokumen7 halamanCholinergic Drugs - TablesThuan Tăng NguyenBelum ada peringkat
- Practical Guide to Urinalysis Screening and InterpretationDokumen9 halamanPractical Guide to Urinalysis Screening and InterpretationyuppierajBelum ada peringkat
- Antiemetic Drugs PDFDokumen12 halamanAntiemetic Drugs PDFDanisha Laila100% (2)
- Drug StudyDokumen3 halamanDrug StudyGena Manimtim100% (1)
- Pharmacist's Letter: Prescriber's LetterDokumen6 halamanPharmacist's Letter: Prescriber's LetterJaved AkhtarBelum ada peringkat
- Pharm 4 Fun Suzanne Morris MetronidazoleDokumen2 halamanPharm 4 Fun Suzanne Morris MetronidazoleJasmyn RoseBelum ada peringkat
- Anti Tubercular DrugsDokumen63 halamanAnti Tubercular DrugsYasir KhanBelum ada peringkat
- Oxytocin and Methylergonovine Nursing StudyDokumen16 halamanOxytocin and Methylergonovine Nursing StudyDinarkram Rabreca EculBelum ada peringkat
- Generic Name: BudesonideDokumen8 halamanGeneric Name: BudesonidemeangelmeBelum ada peringkat
- Chapter 13 PharmacologyDokumen35 halamanChapter 13 PharmacologyEdelrose LapitanBelum ada peringkat
- Drugs Affecting the Respiratory SystemDokumen137 halamanDrugs Affecting the Respiratory SystemUmar Bakshi100% (1)
- Complete Drugs StudyDokumen13 halamanComplete Drugs StudyPeace Andong PerochoBelum ada peringkat
- Pharmocology Drug Cards: InnovarDokumen33 halamanPharmocology Drug Cards: InnovarfaizaBelum ada peringkat
- Drug Study Pyrantel & CefuroximeDokumen2 halamanDrug Study Pyrantel & CefuroximeMikhael Briones ApasBelum ada peringkat
- Anticoagulants DrugsDokumen6 halamanAnticoagulants DrugsHusam Al-OdatBelum ada peringkat
- Tiotropium uses and side effectsDokumen2 halamanTiotropium uses and side effectsjulieBelum ada peringkat
- Chemotherapeutic DrugsDokumen122 halamanChemotherapeutic Drugsdex7reme100% (1)
- Antibiotic Class by CoverageDokumen3 halamanAntibiotic Class by Coverageayy1Belum ada peringkat
- Predisposing Factors of ADRsDokumen7 halamanPredisposing Factors of ADRssuhas reddyBelum ada peringkat
- Antiviral AgentsDokumen14 halamanAntiviral AgentsKate MendozaBelum ada peringkat
- Pharmacotherapy of - Benign Prostatic HyperplasiaDokumen4 halamanPharmacotherapy of - Benign Prostatic HyperplasiaBaarid HamidiBelum ada peringkat
- Management of Tuberculosis: A guide for clinicians (eBook edition)Dari EverandManagement of Tuberculosis: A guide for clinicians (eBook edition)Belum ada peringkat
- A Simple Guide to Abdominal Aortic Aneurysm, Diagnosis, Treatment and Related ConditionsDari EverandA Simple Guide to Abdominal Aortic Aneurysm, Diagnosis, Treatment and Related ConditionsBelum ada peringkat
- Inflamed Trachea, (Tracheitis) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDari EverandInflamed Trachea, (Tracheitis) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsBelum ada peringkat
- Pharmacotherapy of Peptic Ulcer: DR ZareenDokumen50 halamanPharmacotherapy of Peptic Ulcer: DR ZareenGareth BaleBelum ada peringkat
- Pharmacotherapy of Peptic Ulcer: Classification and Mechanisms of DrugsDokumen50 halamanPharmacotherapy of Peptic Ulcer: Classification and Mechanisms of DrugsGareth BaleBelum ada peringkat
- Pharmacology of The Gastrointestinal Drugs (I)Dokumen12 halamanPharmacology of The Gastrointestinal Drugs (I)anaBelum ada peringkat
- Drug CardsDokumen17 halamanDrug CardsJoane LacapBelum ada peringkat
- Prperman 2016 14 3 (Spec. 14Dokumen8 halamanPrperman 2016 14 3 (Spec. 14celia rifaBelum ada peringkat
- Chapter-5 Contract ManagementDokumen43 halamanChapter-5 Contract Managementprem kumarBelum ada peringkat
- Project Cost ForecastDokumen11 halamanProject Cost ForecastJames MendesBelum ada peringkat
- Classification of MatterDokumen2 halamanClassification of Matterapi-280247238Belum ada peringkat
- Seismic Design Guide (2010)Dokumen102 halamanSeismic Design Guide (2010)ingcarlosgonzalezBelum ada peringkat
- 2022 - J - Chir - Nastase Managementul Neoplaziilor Pancreatice PapilareDokumen8 halaman2022 - J - Chir - Nastase Managementul Neoplaziilor Pancreatice PapilarecorinaBelum ada peringkat
- Description MicroscopeDokumen4 halamanDescription MicroscopeRanma SaotomeBelum ada peringkat
- The Ideal Structure of ZZ (Alwis)Dokumen8 halamanThe Ideal Structure of ZZ (Alwis)yacp16761Belum ada peringkat
- Utilization of Wood WasteDokumen14 halamanUtilization of Wood WasteSalman ShahzadBelum ada peringkat
- Mohammad R. Mestarihi: About Me ObjectiveDokumen1 halamanMohammad R. Mestarihi: About Me ObjectiveMhmd MsttBelum ada peringkat
- Hearing God Through Biblical Meditation - 1 PDFDokumen20 halamanHearing God Through Biblical Meditation - 1 PDFAlexander PeñaBelum ada peringkat
- "The Meeting of Meditative Disciplines and Western Psychology" Roger Walsh Shauna L. ShapiroDokumen13 halaman"The Meeting of Meditative Disciplines and Western Psychology" Roger Walsh Shauna L. ShapiroSayako87Belum ada peringkat
- Roxas Avenue, Isabela City, Basilan Province AY: 2018-2019: Claret College of IsabelaDokumen2 halamanRoxas Avenue, Isabela City, Basilan Province AY: 2018-2019: Claret College of IsabelaJennilyn omnosBelum ada peringkat
- Broom Manufacture Machine: StartDokumen62 halamanBroom Manufacture Machine: StartHaziq PazliBelum ada peringkat
- Vernacular Architecture: Bhunga Houses, GujaratDokumen12 halamanVernacular Architecture: Bhunga Houses, GujaratArjun GuptaBelum ada peringkat
- Educating The PosthumanDokumen50 halamanEducating The PosthumanCatherine BrugelBelum ada peringkat
- PoiconverterDokumen2 halamanPoiconvertertaco6541Belum ada peringkat
- Graphs & Charts SummariesDokumen20 halamanGraphs & Charts SummariesMaj Ma Salvador-Bandiola100% (1)
- CPS Layoffs BreakdownDokumen21 halamanCPS Layoffs BreakdownjroneillBelum ada peringkat
- Makerwys - Exe Version 4.891: by Pete Dowson © 2019 InstructionsDokumen11 halamanMakerwys - Exe Version 4.891: by Pete Dowson © 2019 InstructionsRafrol RamonBelum ada peringkat
- Biosynthesis of FlavoursDokumen9 halamanBiosynthesis of FlavoursDatta JoshiBelum ada peringkat
- Valentine Gifting - Accessories EditionDokumen25 halamanValentine Gifting - Accessories EditionPriyanath PaulBelum ada peringkat
- Case Analysis of CriminologyDokumen12 halamanCase Analysis of CriminologyinderpreetBelum ada peringkat
- Pub - Perspectives On Global Cultures Issues in Cultural PDFDokumen190 halamanPub - Perspectives On Global Cultures Issues in Cultural PDFCherlyn Jane Ventura TuliaoBelum ada peringkat
- Pahang JUJ 2012 SPM ChemistryDokumen285 halamanPahang JUJ 2012 SPM ChemistryJeyShida100% (1)
- Liugong 938 Wheel Loader Parts ManualDokumen20 halamanLiugong 938 Wheel Loader Parts Manualjonathan100% (49)
- Analogue Lab Manual AL7212 V2.1-Panduan Praktek DSR Elektronika-DikonversiDokumen235 halamanAnalogue Lab Manual AL7212 V2.1-Panduan Praktek DSR Elektronika-DikonversiAl-FarabiBelum ada peringkat
- Resp Part 4Dokumen95 halamanResp Part 4Kristian CadaBelum ada peringkat
- Product Differentiation and Market Segmentation As Alternative Marketing StrategiesDokumen7 halamanProduct Differentiation and Market Segmentation As Alternative Marketing StrategiesCaertiMBelum ada peringkat
- Appraisal Sample PDFDokumen22 halamanAppraisal Sample PDFkiruthikaBelum ada peringkat