Anda mungkin juga menyukai
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5795)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- This Tutorial Will Help To Test The Throttle Position Sensor On Your 1989 To 1997 1Dokumen7 halamanThis Tutorial Will Help To Test The Throttle Position Sensor On Your 1989 To 1997 1HERBERT SITORUS100% (1)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- Talk - Data Quality FrameworkDokumen30 halamanTalk - Data Quality FrameworkMatthew LawlerBelum ada peringkat
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- FBL ManualDokumen12 halamanFBL Manualaurumstar2000Belum ada peringkat
- SQA Plan TemplateDokumen105 halamanSQA Plan Templatestudent1291Belum ada peringkat
- EAU 2022 - Prostate CancerDokumen229 halamanEAU 2022 - Prostate Cancerpablo penguinBelum ada peringkat
- LTE Radio Network Design Guideline (FDD)Dokumen33 halamanLTE Radio Network Design Guideline (FDD)Tri Frida NingrumBelum ada peringkat
- Dungeon Magazine 195 PDFDokumen5 halamanDungeon Magazine 195 PDFGuillaumeRicherBelum ada peringkat
- Triptico NIC 16Dokumen3 halamanTriptico NIC 16Brayan HMBelum ada peringkat
- CRM Short QuizDokumen1 halamanCRM Short QuizDaria Par-HughesBelum ada peringkat
- Case Study 1Dokumen2 halamanCase Study 1asad ee100% (1)
- Maintenance Repair Overhaul: Safely To New Horizons Ensuring Your Aircraft Is Ready Whenever Duty CallsDokumen10 halamanMaintenance Repair Overhaul: Safely To New Horizons Ensuring Your Aircraft Is Ready Whenever Duty CallsSuryaBelum ada peringkat
- Winter 2016 QP3 Spreadsheet QuestionDokumen2 halamanWinter 2016 QP3 Spreadsheet Questioneegeekeek eieoieeBelum ada peringkat
- School MemoDokumen1 halamanSchool MemoBellaBelum ada peringkat
- Lust V Animal Logic MSJ OppositionDokumen34 halamanLust V Animal Logic MSJ OppositionTHROnlineBelum ada peringkat
- Cronbach's AlphaDokumen4 halamanCronbach's AlphaHeide Orevillo Apa-apBelum ada peringkat
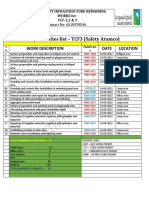
- Daily Activities List - TCF3 (Safety Aramco) : Work Description Date LocationDokumen2 halamanDaily Activities List - TCF3 (Safety Aramco) : Work Description Date LocationSheri DiĺlBelum ada peringkat
- 02 - STD - Bimetal Overload Relay - (2.07 - 2.08)Dokumen2 halaman02 - STD - Bimetal Overload Relay - (2.07 - 2.08)ThilinaBelum ada peringkat
- 6 CHDokumen27 halaman6 CHjafariBelum ada peringkat
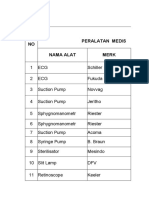
- Daftar Kalibrasi Peralatan MedisDokumen34 halamanDaftar Kalibrasi Peralatan Medisdiklat rssnBelum ada peringkat
- Rhea Huddleston For Supervisor - 17467 - DR2Dokumen1 halamanRhea Huddleston For Supervisor - 17467 - DR2Zach EdwardsBelum ada peringkat
- Tween 80 CoADokumen1 halamanTween 80 CoATấn Huy HồBelum ada peringkat
- Orphanage Project ProposalDokumen3 halamanOrphanage Project ProposaldtimtimanBelum ada peringkat
- Taifun GT User GuideDokumen5 halamanTaifun GT User GuidecarloslarumbeBelum ada peringkat
- PV1800VPM SEREIS (1-5KW) : Pure Sine Wave High Frequency Solar Inverter With MPPT InsideDokumen4 halamanPV1800VPM SEREIS (1-5KW) : Pure Sine Wave High Frequency Solar Inverter With MPPT InsideHuber CallataBelum ada peringkat
- Vol 17 No 3 and No 4 Fort Laramie and The Sioux War of 1876Dokumen19 halamanVol 17 No 3 and No 4 Fort Laramie and The Sioux War of 1876Лазар СрећковићBelum ada peringkat
- PepsiCo Strategic Plan Design PDFDokumen71 halamanPepsiCo Strategic Plan Design PDFdemereBelum ada peringkat
- Pas 38 Pas 41 Pas 40Dokumen12 halamanPas 38 Pas 41 Pas 40Leddie Bergs Villanueva VelascoBelum ada peringkat
- Activity Diagram 1Dokumen14 halamanActivity Diagram 1Yousef GamalBelum ada peringkat
- Ems Accounting Term 2Dokumen39 halamanEms Accounting Term 2Paballo KoopediBelum ada peringkat
- OS Lab ManualDokumen37 halamanOS Lab ManualVenkatanagasudheer ThummapudiBelum ada peringkat