Anda mungkin juga menyukai
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Kaplan Medical Residency GuideDokumen12 halamanKaplan Medical Residency GuideBachelordocBelum ada peringkat
- Dao Ma Mahar PDFDokumen364 halamanDao Ma Mahar PDFdanny100% (15)
- Knee Examination - OSCE SkillsDokumen3 halamanKnee Examination - OSCE Skillsfranksmith51Belum ada peringkat
- PSGS Eligibility Form 2 - Tabulation of Cases 2024Dokumen3 halamanPSGS Eligibility Form 2 - Tabulation of Cases 2024polkadatuinBelum ada peringkat
- Permissive AuthoriatDokumen2 halamanPermissive AuthoriatReiki KiranBelum ada peringkat
- Tan No:Blrc08567G Draft Pay Bill Not To Submit To: Government of KarnatakaDokumen2 halamanTan No:Blrc08567G Draft Pay Bill Not To Submit To: Government of KarnatakavivekbaroleBelum ada peringkat
- Final T An No:B LRT06417F Pay Bill To Be Pre S Ente D TODokumen2 halamanFinal T An No:B LRT06417F Pay Bill To Be Pre S Ente D TOvivekbaroleBelum ada peringkat
- KJJJJDokumen3 halamanKJJJJvivekbaroleBelum ada peringkat
- Income CertificateDokumen1 halamanIncome Certificatevivekbarole100% (1)
- SplintersDokumen4 halamanSplintersvivekbaroleBelum ada peringkat
- Collective Bargaining: Trade Unions Collective Agreements Overtime GrievanceDokumen4 halamanCollective Bargaining: Trade Unions Collective Agreements Overtime GrievancevivekbaroleBelum ada peringkat
- Project On Compitative Anlyses On Depodsitery Service PraviderDokumen59 halamanProject On Compitative Anlyses On Depodsitery Service PravidervivekbaroleBelum ada peringkat
- ChallanDokumen1 halamanChallanvivekbaroleBelum ada peringkat
- Ada 15Dokumen16 halamanAda 15vivekbaroleBelum ada peringkat
- Snellen Eye ChartDokumen2 halamanSnellen Eye ChartTaimoorMirBelum ada peringkat
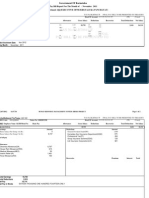
- Healthcare Product Comparison System Titles ReportDokumen1 halamanHealthcare Product Comparison System Titles ReportHector AudelloBelum ada peringkat
- The Cesarean Section Rate in Cases With Premature Rupture of Membrane (Prom) at 36Th Week of Pregnancy or LaterDokumen5 halamanThe Cesarean Section Rate in Cases With Premature Rupture of Membrane (Prom) at 36Th Week of Pregnancy or LaterBob IrsanBelum ada peringkat
- Oefc 1 - 1Dokumen6 halamanOefc 1 - 1Mimi KeceBelum ada peringkat
- Shoulder - Shoulder ImpingementDokumen13 halamanShoulder - Shoulder ImpingementMhmd IrakyBelum ada peringkat
- Signal Review Panel Under PvPI PDFDokumen3 halamanSignal Review Panel Under PvPI PDFAnju ThejkumarBelum ada peringkat
- Dr. Praveen PresentationDokumen63 halamanDr. Praveen PresentationPraveen KumarBelum ada peringkat
- NUR195 ADokumen14 halamanNUR195 AJemuel DalanaBelum ada peringkat
- Courtney Harmon Leadership ResumeDokumen2 halamanCourtney Harmon Leadership Resumeapi-482580060Belum ada peringkat
- Premature Rupture of MembranesDokumen4 halamanPremature Rupture of MembranesRobiyanti Nur Chalifah HattaBelum ada peringkat
- AwwwwwwwwwwwwwwwwwwwwwwwwwwwwwwwwDokumen22 halamanAwwwwwwwwwwwwwwwwwwwwwwwwwwwwwwwwRamon Chito S. PudelananBelum ada peringkat
- Glomerular Diseases in Pregnancy - Kidney (2023)Dokumen18 halamanGlomerular Diseases in Pregnancy - Kidney (2023)cheve glzBelum ada peringkat
- Guideline For The Evaluation and Management of Patients With SyncopeDokumen99 halamanGuideline For The Evaluation and Management of Patients With SyncopePhúc Thiện NguyễnBelum ada peringkat
- Vladimiras Chijenas - NRS in Newborn InfantsDokumen31 halamanVladimiras Chijenas - NRS in Newborn InfantsFausiah Ulva MBelum ada peringkat
- D.R. Form Actual Delivery Form: Brgy. 16-S Quiling Sur, Batac City (077) 670-1920Dokumen8 halamanD.R. Form Actual Delivery Form: Brgy. 16-S Quiling Sur, Batac City (077) 670-1920Fleo GardivoBelum ada peringkat
- CANMAT 2016 Section 6. Special Populations Youth, Women and ElderlyDokumen16 halamanCANMAT 2016 Section 6. Special Populations Youth, Women and ElderlyPablo NuñezBelum ada peringkat
- TeresaDokumen2 halamanTeresaapi-435131948Belum ada peringkat
- MLC Protocols and Its Awareness Among Dental Professionals - A ReviewDokumen4 halamanMLC Protocols and Its Awareness Among Dental Professionals - A ReviewInternational Journal of Innovative Science and Research TechnologyBelum ada peringkat
- INA2Dokumen6 halamanINA2aang_freakBelum ada peringkat
- Public Health Affiliation ReportDokumen36 halamanPublic Health Affiliation ReportAustine AmehBelum ada peringkat
- Senate Bill No 2635Dokumen5 halamanSenate Bill No 2635CBCP for LifeBelum ada peringkat
- Australian Journal of Advanced Nursing: in This IssueDokumen69 halamanAustralian Journal of Advanced Nursing: in This IssueasepBelum ada peringkat
- Acute Management of Nephrolithiasis in Children - UpToDateDokumen15 halamanAcute Management of Nephrolithiasis in Children - UpToDatedrtgodeBelum ada peringkat
- Embolismo Pulmonar NejmDokumen3 halamanEmbolismo Pulmonar NejmSaidBelum ada peringkat
- NiSchool - PaediatricsDokumen48 halamanNiSchool - PaediatricsNurul Izzah AzmiBelum ada peringkat