Anda mungkin juga menyukai
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- CSTR Excel Model TemplateDokumen83 halamanCSTR Excel Model TemplatefitzggBelum ada peringkat
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Complete Notes On 9th Physics by Asif RasheedDokumen82 halamanComplete Notes On 9th Physics by Asif RasheedAsif Rasheed Rajput75% (28)
- Mechanical Properties OF Dental MaterialsDokumen40 halamanMechanical Properties OF Dental MaterialsRamnarayan MeenaBelum ada peringkat
- Management of Dilacerated and S-ShapedDokumen3 halamanManagement of Dilacerated and S-ShapedRăican AlexandruBelum ada peringkat
- Management of Dilacerated and S-ShapedDokumen3 halamanManagement of Dilacerated and S-ShapedRăican AlexandruBelum ada peringkat
- Endodontic Treatment of Curved Root Canal Systems PDFDokumen3 halamanEndodontic Treatment of Curved Root Canal Systems PDFRăican AlexandruBelum ada peringkat
- Glide Path in Endodontics PDFDokumen6 halamanGlide Path in Endodontics PDFRăican AlexandruBelum ada peringkat
- SJ - BDJ .2013.379Dokumen6 halamanSJ - BDJ .2013.379Vimi GeorgeBelum ada peringkat
- Chap 4Dokumen18 halamanChap 4api-3702256100% (2)
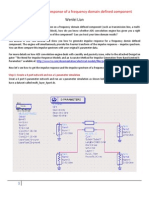
- Impulse Response of Frequency Domain ComponentDokumen17 halamanImpulse Response of Frequency Domain Componentbubo28Belum ada peringkat
- Mechanics of Solids Lab ManualDokumen47 halamanMechanics of Solids Lab Manualravi03319100% (1)
- Week - 7 - Analysis - of - State - Space - SystemsDokumen32 halamanWeek - 7 - Analysis - of - State - Space - SystemsMetin DurmuşBelum ada peringkat
- Various Types of Surfaces: Made By:-Nilesh Bhojani Guided By: - Prof. B.K. PatelDokumen15 halamanVarious Types of Surfaces: Made By:-Nilesh Bhojani Guided By: - Prof. B.K. Patelnilesh bhojaniBelum ada peringkat
- Chapter 2 Process ControllDokumen29 halamanChapter 2 Process ControllWeldush BrightBelum ada peringkat
- Vibration Analysis, Control and Optimum Accelerometer Placement For Successful Vibrations TestsDokumen44 halamanVibration Analysis, Control and Optimum Accelerometer Placement For Successful Vibrations TestsVyankatesh AshtekarBelum ada peringkat
- Integration Atmospheric Stability CFD Modeling MeteodynWT For Wind Resource Assessment AEP Validation Real Case Wind FarmDokumen1 halamanIntegration Atmospheric Stability CFD Modeling MeteodynWT For Wind Resource Assessment AEP Validation Real Case Wind FarmMeteodyn_EnergyBelum ada peringkat
- First Principles Determination of Elastic Constants and Chemical Bonding of Titanium Boride (TiB) On The Basis of Density Functional TheoryDokumen17 halamanFirst Principles Determination of Elastic Constants and Chemical Bonding of Titanium Boride (TiB) On The Basis of Density Functional Theoryjianqi199808Belum ada peringkat
- 1st Grading Performance TestDokumen4 halaman1st Grading Performance TestMary Ann GellorExito EvarolaBelum ada peringkat
- Pengaruh Kandungan Frekuensi Gempa Terhadap Simpangan Dan Drift Ratio 2 Arah Struktur Bangunan Set-Back Bertingkat BanyakDokumen9 halamanPengaruh Kandungan Frekuensi Gempa Terhadap Simpangan Dan Drift Ratio 2 Arah Struktur Bangunan Set-Back Bertingkat BanyakIvan MuhammadBelum ada peringkat
- Robinson VacDokumen10 halamanRobinson VacJajajaBelum ada peringkat
- Journey To The Edge of ReasonDokumen337 halamanJourney To The Edge of ReasonFrancesco CavinaBelum ada peringkat
- Keeara Walji - Fri April 30 - Mon April 3 - Exploration Lesson 2Dokumen11 halamanKeeara Walji - Fri April 30 - Mon April 3 - Exploration Lesson 2Keeara WaljiBelum ada peringkat
- Ko 2015Dokumen22 halamanKo 2015Mudavath Babu RamBelum ada peringkat
- PPSD A TT 027 0002 R0Dokumen14 halamanPPSD A TT 027 0002 R0santosh_ms_kumar2827Belum ada peringkat
- Cauchy Riemann EquationDokumen6 halamanCauchy Riemann EquationeSinist3rBelum ada peringkat
- Terminology of Helical SpringDokumen4 halamanTerminology of Helical Springsandeep c sBelum ada peringkat
- Determination of Dissolved Oxygen in Sea Water by Winkler TitrationDokumen11 halamanDetermination of Dissolved Oxygen in Sea Water by Winkler TitrationEstBelum ada peringkat
- MVC-FD83 / FD88 Service ManualDokumen113 halamanMVC-FD83 / FD88 Service ManualImraan RamdjanBelum ada peringkat
- Millman and Parker - Geometry - A Metric PDFDokumen388 halamanMillman and Parker - Geometry - A Metric PDFallan13080% (5)
- Soil Science: Classification of PedologyDokumen24 halamanSoil Science: Classification of Pedologyekush amar100% (1)
- Sulpiride MonographieDokumen3 halamanSulpiride MonographieMohamed DahmaneBelum ada peringkat
- 55 4 2 PhysicsDokumen27 halaman55 4 2 PhysicsSriramBelum ada peringkat
- WT Chapter 6 2Dokumen21 halamanWT Chapter 6 2kanchanabalajiBelum ada peringkat
- Iec STD ListsDokumen6 halamanIec STD Listssasenthil241464Belum ada peringkat
- 5.2 Production Facilities PDFDokumen110 halaman5.2 Production Facilities PDFJohn Cooper100% (5)