Anda mungkin juga menyukai
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- FEYNMAN, Richard. What-Do-You-Care-What-Other-People-Think PDFDokumen111 halamanFEYNMAN, Richard. What-Do-You-Care-What-Other-People-Think PDFFELLINIERS100% (2)
- Electric Circuit Analysis PDFDokumen53 halamanElectric Circuit Analysis PDFmasimeriseBelum ada peringkat
- Hydrogen-Induced Cracking Susceptibility in High-Strength Weld MetalDokumen6 halamanHydrogen-Induced Cracking Susceptibility in High-Strength Weld MetalgrandecaciqueBelum ada peringkat
- Scanning Electron MicrosDokumen55 halamanScanning Electron MicrosAnson Chan100% (1)
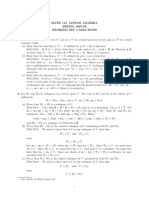
- Math110s Hw2solDokumen4 halamanMath110s Hw2solankitBelum ada peringkat
- Physics Project: ON EMP JammerDokumen17 halamanPhysics Project: ON EMP JammerAnonymous q9FjgwT5Belum ada peringkat
- CPP (GOC) - NewDokumen4 halamanCPP (GOC) - Newpankaj16fbBelum ada peringkat
- Feedback - Week 3 QuizDokumen6 halamanFeedback - Week 3 QuizjcvoscribBelum ada peringkat
- Agitation and MixingDokumen77 halamanAgitation and MixingKolliparaDeepak100% (1)
- GE6253 - ENGINEERING MECHANICS - Unit 5 Friction - LECTURE NOTESDokumen26 halamanGE6253 - ENGINEERING MECHANICS - Unit 5 Friction - LECTURE NOTESstkrBelum ada peringkat
- Procedures For The Analysis of Explosives EvidenceDokumen15 halamanProcedures For The Analysis of Explosives EvidenceGerman CarleBelum ada peringkat
- Tanker Analiz RaporuDokumen23 halamanTanker Analiz Raporuakın ersözBelum ada peringkat
- Lecture C-Open MappingDokumen6 halamanLecture C-Open Mappingarnav mishraBelum ada peringkat
- G484 Jan 11Dokumen12 halamanG484 Jan 11samy9387Belum ada peringkat
- Fluid Mechanics (6Th Ed.), Frank M. White, Mcgraw Hill, 2007Dokumen4 halamanFluid Mechanics (6Th Ed.), Frank M. White, Mcgraw Hill, 2007cartoon_nate100% (1)
- Coulombs LawDokumen22 halamanCoulombs LawSam HeartsBelum ada peringkat
- Science 8: Learning Activity Sheet inDokumen12 halamanScience 8: Learning Activity Sheet inJoan MarieBelum ada peringkat
- XYZ Dairy EnggDokumen7 halamanXYZ Dairy EnggBhuwesh PantBelum ada peringkat
- Investigation of Fine Structure of Textile FibreDokumen12 halamanInvestigation of Fine Structure of Textile FibreSuyash Manmohan100% (1)
- VSEPRDokumen1 halamanVSEPRĐan KhanhBelum ada peringkat
- Particle Size of Granules and Mechanical Properties of Paracetamol TabletsDokumen3 halamanParticle Size of Granules and Mechanical Properties of Paracetamol TabletsAdnanBelum ada peringkat
- Differential Analysis of Fluid Flow 1221Dokumen120 halamanDifferential Analysis of Fluid Flow 1221Waqar A. KhanBelum ada peringkat
- Class Xii - Physics - Mock Test - 1 (Obj) - 09.11.2021Dokumen6 halamanClass Xii - Physics - Mock Test - 1 (Obj) - 09.11.2021Sankar KumarasamyBelum ada peringkat
- Supply Air DiffuserDokumen6 halamanSupply Air Diffuserntt_121987Belum ada peringkat
- Relativity: Relativity Deals With Measurement of Events: Where and When They Happen, andDokumen23 halamanRelativity: Relativity Deals With Measurement of Events: Where and When They Happen, andAngelica LlamasBelum ada peringkat
- Chem Covalent Bond 2Dokumen53 halamanChem Covalent Bond 2Erica Joy UngriaBelum ada peringkat
- Chapter 23 Non-Destructive Testing of Hardened ConcreteDokumen6 halamanChapter 23 Non-Destructive Testing of Hardened Concretemusiomi2005Belum ada peringkat
- Steel Chap5 Ultimate Limit StateDokumen35 halamanSteel Chap5 Ultimate Limit StateMesfin Derbew86% (7)