Anda mungkin juga menyukai
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- IR Light Therapy PDFDokumen97 halamanIR Light Therapy PDFcamarondelaisla100% (3)
- Hypothyroidism and ThyroiditisDokumen35 halamanHypothyroidism and ThyroiditisXochil RmzBelum ada peringkat
- Art 3A10.1007 2Fs00259 013 2535 3 PDFDokumen477 halamanArt 3A10.1007 2Fs00259 013 2535 3 PDFHerryAsu-songkoBelum ada peringkat
- Cme Endocrinology Saqs (80447) : Self-Assessment QuestionnaireDokumen3 halamanCme Endocrinology Saqs (80447) : Self-Assessment QuestionnaireAbu AhmedBelum ada peringkat
- Enf Tiroidea y Embarazo Lancet 2018Dokumen12 halamanEnf Tiroidea y Embarazo Lancet 2018Jair Alexander Quintero PanucoBelum ada peringkat
- 70 Years of LevothyroxineDokumen141 halaman70 Years of LevothyroxinecavrisBelum ada peringkat
- Cretenism Case StudyDokumen8 halamanCretenism Case StudyMonica Marie MoralesBelum ada peringkat
- Bhs Inggris PerbaikanDokumen4 halamanBhs Inggris PerbaikanDolly cupingBelum ada peringkat
- Anatomy and Physiology of ThyroidDokumen74 halamanAnatomy and Physiology of ThyroidSajid NadafBelum ada peringkat
- Magnetic Resonance Imaging Versus Serum Iron Status As Diagnostic Tools For Pituitary Iron Overload in Children With Beta ThalassemiaDokumen13 halamanMagnetic Resonance Imaging Versus Serum Iron Status As Diagnostic Tools For Pituitary Iron Overload in Children With Beta ThalassemiaAbdurrahman HasanuddinBelum ada peringkat
- 2nd Journal - Andre Parmonangan Panjaitan - 013Dokumen7 halaman2nd Journal - Andre Parmonangan Panjaitan - 013Andre Parmonangan PanjaitanBelum ada peringkat
- DissertationDokumen88 halamanDissertationShohida NaimovaBelum ada peringkat
- Hormones and Related DrugsDokumen42 halamanHormones and Related DrugsRamya PrabhuBelum ada peringkat
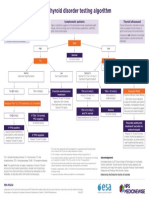
- NPS MedicineWise Thyroid Testing Algorithm v3Dokumen1 halamanNPS MedicineWise Thyroid Testing Algorithm v3Mikhael JHBelum ada peringkat
- Endocrine HarmonyDokumen68 halamanEndocrine HarmonyafnanBelum ada peringkat
- ОВБ-2 Ответы фулDokumen70 halamanОВБ-2 Ответы фулMoldir AkynbayBelum ada peringkat
- Common Drugs To ExplainDokumen2 halamanCommon Drugs To ExplainJeemeenee Haerim SonBelum ada peringkat
- Management of of Clients With Metabolic and EndocrineDokumen79 halamanManagement of of Clients With Metabolic and Endocrineagbogoodness100% (1)
- Title: Congenital Hypothyroidism: A Ran Sacker Escaping Under The Nose AbstractDokumen6 halamanTitle: Congenital Hypothyroidism: A Ran Sacker Escaping Under The Nose AbstractKavita KhannaBelum ada peringkat
- Nursing Practice Test - EndocrineDokumen20 halamanNursing Practice Test - Endocrinemay17sanchez100% (7)
- Endocrine, Metabolic & Nephrology MCQS: Thyroid Eye DiseaseDokumen78 halamanEndocrine, Metabolic & Nephrology MCQS: Thyroid Eye DiseaseDr.younes95 RekaaneyBelum ada peringkat
- The Prevalence of Anti-Thyroid Peroxidase Antibodies and Autoimmune Thyroiditis in Children and Adolescents in An Iodine Replete AreaDokumen7 halamanThe Prevalence of Anti-Thyroid Peroxidase Antibodies and Autoimmune Thyroiditis in Children and Adolescents in An Iodine Replete AreaAkshay BankayBelum ada peringkat
- Thyroid Benign TumorDokumen30 halamanThyroid Benign TumormackieccBelum ada peringkat
- Endocrin E Diseases: by Group 3Dokumen53 halamanEndocrin E Diseases: by Group 3Ash AshBelum ada peringkat
- Pediatric in ReviewDokumen10 halamanPediatric in ReviewkafosidBelum ada peringkat
- Pathologic Conditios of Endocrine Disorder.Dokumen42 halamanPathologic Conditios of Endocrine Disorder.ramoli1988Belum ada peringkat
- BHTbook StevenWmFowkes 141016Dokumen67 halamanBHTbook StevenWmFowkes 141016Sparklight JackBelum ada peringkat
- Hypothyroidism Case AnalysisDokumen3 halamanHypothyroidism Case AnalysisKrisianne Mae Lorenzo FranciscoBelum ada peringkat
- Armour Thyroid (Thyroid Tablets, USP) RX Only: I I NHDokumen10 halamanArmour Thyroid (Thyroid Tablets, USP) RX Only: I I NHAdam GolsbyBelum ada peringkat
- Thyroid Case StudyDokumen68 halamanThyroid Case Studyshadydogv5Belum ada peringkat