Anda mungkin juga menyukai
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Social Support and Stress ToleranceDokumen4 halamanSocial Support and Stress Toleranceesinu27Belum ada peringkat
- Attitude and Aptitude Towards Teaching Performance of Teacher Educators in B.ed CollegesDokumen4 halamanAttitude and Aptitude Towards Teaching Performance of Teacher Educators in B.ed CollegesAnonymous CwJeBCAXpBelum ada peringkat
- Anya S. Salik G12-STEM - Sison Understanding Culture, Society and Politics Quarter 1 - Module 5Dokumen3 halamanAnya S. Salik G12-STEM - Sison Understanding Culture, Society and Politics Quarter 1 - Module 5Naila SalikBelum ada peringkat
- Leadership in Project ManagementDokumen17 halamanLeadership in Project ManagementPrithwi MukherjeeBelum ada peringkat
- You Are ResponsibleDokumen12 halamanYou Are ResponsibleDharma Daana100% (1)
- XOJane - My Former Friend's Death Was A Blessing - Amanda LaurenDokumen5 halamanXOJane - My Former Friend's Death Was A Blessing - Amanda LaurenMatthew Keys100% (3)
- Bakhurst, Shanker - 2001 - Jerome Bruner Culture Language and SelfDokumen349 halamanBakhurst, Shanker - 2001 - Jerome Bruner Culture Language and SelfAlejandro León100% (1)
- Developing Professional CapacityDokumen6 halamanDeveloping Professional Capacityapi-476189522Belum ada peringkat
- Trauma For Parent Groups 10 - 10 - 19Dokumen44 halamanTrauma For Parent Groups 10 - 10 - 19Htet HtinBelum ada peringkat
- Gender ContinuumDokumen3 halamanGender ContinuumTrisha MariehBelum ada peringkat
- Adult Cognitive AssessmentDokumen15 halamanAdult Cognitive AssessmentClaudia Delia Foltun0% (2)
- A Study On Stress Management: "Master of Business Administration"Dokumen73 halamanA Study On Stress Management: "Master of Business Administration"mohdgazzali71% (7)
- Exceptional MemoryDokumen9 halamanExceptional MemoryDoina MiruzarBelum ada peringkat
- SOJOURNERDokumen2 halamanSOJOURNERJam Concepcion OdoñoBelum ada peringkat
- Ndamani 2008 Factors Contributing To Lack of Discipline in Selected Secondary Schools in The Mangaung Area ofDokumen21 halamanNdamani 2008 Factors Contributing To Lack of Discipline in Selected Secondary Schools in The Mangaung Area ofKathleen SergioBelum ada peringkat
- Business PsychologyDokumen10 halamanBusiness PsychologySami YessBelum ada peringkat
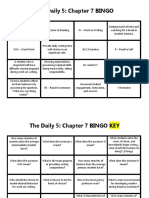
- The Daily 5 Chapter 7 BingoDokumen2 halamanThe Daily 5 Chapter 7 Bingoapi-396925527Belum ada peringkat
- The Filipino Self and The KapwaDokumen3 halamanThe Filipino Self and The KapwaJohn Bryan Languido100% (1)
- Emotional EquanimityDokumen22 halamanEmotional EquanimityRoxy Shira AdiBelum ada peringkat
- Job Characteristics ModelDokumen3 halamanJob Characteristics ModelDipak Thakur0% (1)
- Staff DevelopmentDokumen14 halamanStaff Developmentjoshua alejandroBelum ada peringkat
- A View Behind The Mask of Sanity Meta-Analysis of Aberrant Brain Activity in Psychopaths PDFDokumen8 halamanA View Behind The Mask of Sanity Meta-Analysis of Aberrant Brain Activity in Psychopaths PDFLaura PulidoBelum ada peringkat
- Interpersonal DeceptionDokumen3 halamanInterpersonal DeceptionnizaBelum ada peringkat
- Daring GreatlyDokumen8 halamanDaring Greatlyapi-527676598Belum ada peringkat
- Gestalt Learning TheoryDokumen17 halamanGestalt Learning TheoryJoan BuedoBelum ada peringkat
- Chapter 32Dokumen13 halamanChapter 32slg233Belum ada peringkat
- DomeDokumen86 halamanDomeSiti Nur Hafidzoh Omar100% (1)
- The Factor of IndividualismDokumen2 halamanThe Factor of IndividualismMak GnohodBelum ada peringkat
- 2 - Management of InstructionDokumen15 halaman2 - Management of InstructionMyla Ebillo100% (4)
- Gestalt TherapyDokumen6 halamanGestalt TherapyLily lyka PranillaBelum ada peringkat