Anda mungkin juga menyukai
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (120)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Measurements in EpidemiologyDokumen24 halamanMeasurements in EpidemiologyAnand gowda75% (4)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Baby Massage Consultation Form - November 2017Dokumen1 halamanBaby Massage Consultation Form - November 2017api-257327106Belum ada peringkat
- Jennifer CarrollCV06 17Dokumen11 halamanJennifer CarrollCV06 17jencarr2Belum ada peringkat
- Jennifer CarrollCV06 16Dokumen10 halamanJennifer CarrollCV06 16jencarr2Belum ada peringkat
- Jennifer CarrollCV10 16Dokumen14 halamanJennifer CarrollCV10 16jencarr2Belum ada peringkat
- Jennifer CarrollCV10 16Dokumen14 halamanJennifer CarrollCV10 16jencarr2Belum ada peringkat
- Carroll PerceivedRiskAmongHIV AIDSBehav 2016Dokumen5 halamanCarroll PerceivedRiskAmongHIV AIDSBehav 2016jencarr2Belum ada peringkat
- Jennifer CarrollCV06 16Dokumen12 halamanJennifer CarrollCV06 16jencarr2Belum ada peringkat
- Jennifer CarrollCV04 16Dokumen9 halamanJennifer CarrollCV04 16jencarr2Belum ada peringkat
- PayPal Activity-ASOF-Feb9 2015Dokumen4 halamanPayPal Activity-ASOF-Feb9 2015jencarr2Belum ada peringkat
- For Lack of WantingDokumen19 halamanFor Lack of Wantingjencarr2Belum ada peringkat
- AIDSCare 2016Dokumen8 halamanAIDSCare 2016jencarr2Belum ada peringkat
- Ethnography of The UnexpectedDokumen4 halamanEthnography of The Unexpectedjencarr2Belum ada peringkat
- For Lack of WantingDokumen19 halamanFor Lack of Wantingjencarr2Belum ada peringkat
- 2-Cargo 1-2-11 - 03 CarrollDokumen26 halaman2-Cargo 1-2-11 - 03 Carrolljencarr2Belum ada peringkat
- PoE CarrollDokumen8 halamanPoE Carrolljencarr2Belum ada peringkat
- PayPal - Activity-AUG26 PDFDokumen3 halamanPayPal - Activity-AUG26 PDFjencarr2Belum ada peringkat
- For Lack of WantingDokumen25 halamanFor Lack of Wantingjencarr2Belum ada peringkat
- PayPal - Activity-Aug 4Dokumen3 halamanPayPal - Activity-Aug 4jencarr2Belum ada peringkat
- For Lack of WantingDokumen28 halamanFor Lack of Wantingjencarr2Belum ada peringkat
- TacticalMedic Aug4Dokumen1 halamanTacticalMedic Aug4jencarr2Belum ada peringkat
- Smoking and PEDokumen15 halamanSmoking and PEjencarr2Belum ada peringkat
- ANTH 305 Midterm ReviewDokumen3 halamanANTH 305 Midterm Reviewjencarr2Belum ada peringkat
- ANTH305 Syllabus Carroll SU14Dokumen8 halamanANTH305 Syllabus Carroll SU14jencarr2Belum ada peringkat
- "This Is Not American Heroin": Social Illness, Chemical Therapies, and Biomedical Pluralism in UkraineDokumen11 halaman"This Is Not American Heroin": Social Illness, Chemical Therapies, and Biomedical Pluralism in Ukrainejencarr2Belum ada peringkat
- From The Streets of Kyiv: "We Are Definitely Going Somewhere"Dokumen9 halamanFrom The Streets of Kyiv: "We Are Definitely Going Somewhere"jencarr2Belum ada peringkat
- Anthropology 215 MAGHDokumen10 halamanAnthropology 215 MAGHjencarr2Belum ada peringkat
- Anthropology 101 SeattleDokumen7 halamanAnthropology 101 Seattlejencarr2Belum ada peringkat
- Choosing Methadone ColloquiumDokumen50 halamanChoosing Methadone Colloquiumjencarr2Belum ada peringkat
- SAE Graduate Student Event (AAA 2013)Dokumen1 halamanSAE Graduate Student Event (AAA 2013)jencarr2Belum ada peringkat
- Koch Review PDFDokumen3 halamanKoch Review PDFjencarr2Belum ada peringkat
- Socio - Cultural and Ethnographic Research in Public HealthDokumen33 halamanSocio - Cultural and Ethnographic Research in Public Healthjencarr2Belum ada peringkat
- Sexually Transmitted DiseasesDokumen54 halamanSexually Transmitted DiseasesMowlidAbdirahman Ali madaaleBelum ada peringkat
- CA NursingDokumen5 halamanCA NursingMary Angel Nicka LuayonBelum ada peringkat
- ZIMIND 17 04 2020 P - CompressedDokumen44 halamanZIMIND 17 04 2020 P - CompressedKennedy DubeBelum ada peringkat
- NCP PediatricDokumen5 halamanNCP PediatricSL Hanna NebridaBelum ada peringkat
- WHOOP Health Report Matteo Cerrina Jul 03, 2023Dokumen2 halamanWHOOP Health Report Matteo Cerrina Jul 03, 2023Matteo CerrinaBelum ada peringkat
- Đề 9. Đề thi thử TN THPT môn Tiếng Anh theo cấu trúc đề minh họa 2021 - Cô Oanh 9 - Có lời giảiDokumen14 halamanĐề 9. Đề thi thử TN THPT môn Tiếng Anh theo cấu trúc đề minh họa 2021 - Cô Oanh 9 - Có lời giảiBình Bùi thanhBelum ada peringkat
- Preventive OphthalmologyDokumen2 halamanPreventive Ophthalmologysarguss14100% (1)
- Grand Case Presentation PrepDokumen2 halamanGrand Case Presentation PrepYessamae JinangBelum ada peringkat
- 10.3 - Sensitivity, Specificity, Positive Predictive Value, and Negative Predictive Value - STAT 507Dokumen3 halaman10.3 - Sensitivity, Specificity, Positive Predictive Value, and Negative Predictive Value - STAT 507Avinash sahu100% (1)
- Indonesia Health SectorDokumen84 halamanIndonesia Health SectorBung RandiBelum ada peringkat
- Grape Seed Extract Outperforms Chemo in Killing Advanced Cancer CellsDokumen4 halamanGrape Seed Extract Outperforms Chemo in Killing Advanced Cancer Cellsinfo-501699Belum ada peringkat
- Digeorge Syndrome: 22q11 DELETIONDokumen6 halamanDigeorge Syndrome: 22q11 DELETIONLouie Anne Cardines AnguloBelum ada peringkat
- 10 Questions April 2022 PDFDokumen7 halaman10 Questions April 2022 PDFWongani ZuluBelum ada peringkat
- Gambaran Usia Pada Kejadian Covid-19: Rosyada Elviani Chairil Anwar Rico Januar SitorusDokumen6 halamanGambaran Usia Pada Kejadian Covid-19: Rosyada Elviani Chairil Anwar Rico Januar SitorusRizka ZahroBelum ada peringkat
- Jurnal Kesehatan MentalDokumen6 halamanJurnal Kesehatan MentalRayhan Gymnastiar NasirBelum ada peringkat
- Neuromuscular System 1Dokumen13 halamanNeuromuscular System 1Shimmering MoonBelum ada peringkat
- Mayur 2 CertificateDokumen1 halamanMayur 2 CertificateYo YoBelum ada peringkat
- Diarrhea, Risk For Fluid Volume DeficitDokumen6 halamanDiarrhea, Risk For Fluid Volume DeficitEfzell Dean BangilanBelum ada peringkat
- Seymour Schools Nov 6 COVID LetterDokumen2 halamanSeymour Schools Nov 6 COVID LetterThe Valley IndyBelum ada peringkat
- Answers To ExercisesDokumen19 halamanAnswers To ExercisesBea ValerioBelum ada peringkat
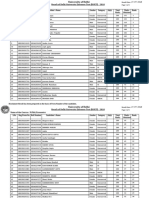
- Name of The Course:-M.Phil, Economics: Result of Delhi University Entrance Test (DUET) - 2018Dokumen5 halamanName of The Course:-M.Phil, Economics: Result of Delhi University Entrance Test (DUET) - 2018Saiganesh RameshBelum ada peringkat
- EDITORIAL Successful Treatment Strategy of Turkey Against Covid19 Outbreak-12345 PDFDokumen2 halamanEDITORIAL Successful Treatment Strategy of Turkey Against Covid19 Outbreak-12345 PDFMohaymin AljabryBelum ada peringkat
- Disease Project Handout and RubricDokumen1 halamanDisease Project Handout and Rubricapi-409240655Belum ada peringkat
- Disease, Signs SymptomsDokumen9 halamanDisease, Signs SymptomsGilang Putra RamadhanBelum ada peringkat
- Herpes GenitalisDokumen13 halamanHerpes GenitalisNataša Ivaniš0% (1)
- Digestive Symptoms in COVID-19 Patients With Mild Disease SeverityDokumen13 halamanDigestive Symptoms in COVID-19 Patients With Mild Disease SeveritytyariBelum ada peringkat
- Therapy LV CNS 4th Year KirubelDokumen156 halamanTherapy LV CNS 4th Year Kirubelpblinder1319Belum ada peringkat
- Parasitology Lecture 1Dokumen84 halamanParasitology Lecture 1Dr Sarah Bakhsh - Resident FCPS Community MedicineBelum ada peringkat