Anda mungkin juga menyukai
- Ab Rehab Guide 2019Dokumen15 halamanAb Rehab Guide 2019maria jose100% (3)
- Spinal Injury Management GuideDokumen60 halamanSpinal Injury Management GuideRheselle LacuataBelum ada peringkat
- Knee Pain and Mobility Impairments: Meniscal and Articular Cartilage LesionsDokumen36 halamanKnee Pain and Mobility Impairments: Meniscal and Articular Cartilage LesionsdedsnetBelum ada peringkat
- Clinical Exam of Hand and Wrist: Guide to Musculoskeletal AssessmentDokumen91 halamanClinical Exam of Hand and Wrist: Guide to Musculoskeletal AssessmentjothiBelum ada peringkat
- HNP CervicalDokumen33 halamanHNP CervicalIndra RanteBelum ada peringkat
- College of Allied Health and SciencesDokumen101 halamanCollege of Allied Health and SciencesArybaa MeerBelum ada peringkat
- Orthopedic Exam Notes Apu PDFDokumen6 halamanOrthopedic Exam Notes Apu PDFabiramirajalaksmiBelum ada peringkat
- Hip ExaminationDokumen84 halamanHip ExaminationDeepak KumarBelum ada peringkat
- Jude's Quadriceps Plasty For Stiff KneeDokumen6 halamanJude's Quadriceps Plasty For Stiff KneeRaviBelum ada peringkat
- Surface AnatomyDokumen318 halamanSurface AnatomymitroisergiuBelum ada peringkat
- September2010 Clinical GuidelinesDokumen26 halamanSeptember2010 Clinical GuidelinesFabianinhoLacerdaBelum ada peringkat
- Hand PDFDokumen179 halamanHand PDFRadenSiwi Bagus HadhiningratBelum ada peringkat
- Tendon Injuries of Hand: DR Saumya AgarwalDokumen101 halamanTendon Injuries of Hand: DR Saumya AgarwaltesfahuntekletilahunBelum ada peringkat
- The Upper Extremity: Sufitni Megasari SitorusDokumen37 halamanThe Upper Extremity: Sufitni Megasari SitorusFakhrur RaziBelum ada peringkat
- Office Orthopaedics: Ramirez, Bryan Paul GDokumen57 halamanOffice Orthopaedics: Ramirez, Bryan Paul GBryan Paul RamirezBelum ada peringkat
- AnkleSprain PCG 27032009Dokumen30 halamanAnkleSprain PCG 27032009Rachel BlackburnBelum ada peringkat
- All CICM Examiner ReportsDokumen432 halamanAll CICM Examiner ReportsHani MikhailBelum ada peringkat
- Plate Fixation in OrthopaedicsDokumen200 halamanPlate Fixation in OrthopaedicsMichael John TedjajuwanaBelum ada peringkat
- ACL and PCL ReconstructionDokumen25 halamanACL and PCL ReconstructionAli Aufar HutasuhutBelum ada peringkat
- Examination of Hand & Common Hand InjuriesDokumen165 halamanExamination of Hand & Common Hand InjuriesPriya GK100% (1)
- Scapula - 18 Muscle AttachmentsDokumen2 halamanScapula - 18 Muscle Attachmentsdarbyje88% (8)
- De Quervain's Tenosynovitis: Dr. Jatin JR3 Year Orthopaed Ics Fmhs Under SGT UniversityDokumen31 halamanDe Quervain's Tenosynovitis: Dr. Jatin JR3 Year Orthopaed Ics Fmhs Under SGT UniversityKuldeep PindariaBelum ada peringkat
- Piriformis Syndrome: A Narrative Review of The Anatomy, Diagnosis, and TreatmentDokumen10 halamanPiriformis Syndrome: A Narrative Review of The Anatomy, Diagnosis, and TreatmentHumairah AnandaBelum ada peringkat
- Jospt LBPDokumen58 halamanJospt LBPHelda PurwaningtiyasBelum ada peringkat
- Anatomy MCQ 1Dokumen15 halamanAnatomy MCQ 1Maria75% (4)
- Posi Appendicular Table NotesDokumen12 halamanPosi Appendicular Table NotesAngelica Montalbo NavaBelum ada peringkat
- Interactions between the Craniomandibular System and Cervical Spine: The influence of an unilateral change of occlusion on the upper cervical range of motionDari EverandInteractions between the Craniomandibular System and Cervical Spine: The influence of an unilateral change of occlusion on the upper cervical range of motionBelum ada peringkat
- Fractures of The Humeral ShaftDokumen25 halamanFractures of The Humeral ShaftMuhammad IqbalBelum ada peringkat
- 22-Surface Anatomy of The Upper and Lower LimbsDokumen24 halaman22-Surface Anatomy of The Upper and Lower LimbsMiahz Tv100% (1)
- Anatomical terms of movementDokumen4 halamanAnatomical terms of movementRica Angelyn AtienzaBelum ada peringkat
- Final FRCA Obstetric Past Questions ResourceDokumen14 halamanFinal FRCA Obstetric Past Questions ResourceMasseh YakubiBelum ada peringkat
- Ulnar Nerve EntrapmentDokumen4 halamanUlnar Nerve Entrapmentnavneetsingh86Belum ada peringkat
- Physical Examination of The Hand: Cme Information and DisclosuresDokumen11 halamanPhysical Examination of The Hand: Cme Information and DisclosuresDesrainy InhardiniBelum ada peringkat
- Carpal Tunnel Syndrome FinalDokumen4 halamanCarpal Tunnel Syndrome Finalcatherine_suganob6496100% (2)
- Tendon TransfersDokumen26 halamanTendon TransfersJohnny Wang100% (1)
- Ultrasound of The Ankle: IndicationsDokumen6 halamanUltrasound of The Ankle: IndicationsElloide PajutanBelum ada peringkat
- Cervicothoracic Regional Exam FindingsDokumen1 halamanCervicothoracic Regional Exam FindingsChristopher NotleyBelum ada peringkat
- 2010 Orthopaedic JournalDokumen80 halaman2010 Orthopaedic JournalPooria1989Belum ada peringkat
- Postural Drainage PositionsDokumen1 halamanPostural Drainage PositionsCheryl100% (1)
- CVM6101 Anatomy SpineDokumen7 halamanCVM6101 Anatomy SpineHéctor LópezBelum ada peringkat
- Spinal Injury & Spinal Cord InjuryDokumen66 halamanSpinal Injury & Spinal Cord InjuryPowool LalaBelum ada peringkat
- Ankle Stability and MovementDokumen40 halamanAnkle Stability and MovementBogdan GeangosBelum ada peringkat
- Using A CaneDokumen1 halamanUsing A CaneCherylBelum ada peringkat
- Musculoskeletal ExaminationDokumen10 halamanMusculoskeletal ExaminationRheeza ElhaqBelum ada peringkat
- JBLMRH - Ortho - Lag Screw TechniqueDokumen17 halamanJBLMRH - Ortho - Lag Screw TechniqueTristan ArellanoBelum ada peringkat
- PNFpresentationDokumen32 halamanPNFpresentationNarkeesh ArumugamBelum ada peringkat
- Clinical Assessment and Examination in Orthopaedics 2nd EditionDokumen4 halamanClinical Assessment and Examination in Orthopaedics 2nd EditionvisfralinBelum ada peringkat
- Osteoarthritis 2018Dokumen45 halamanOsteoarthritis 2018Rizcky Naldy Eka PutraBelum ada peringkat
- Summary MRI Knee ImagingDokumen17 halamanSummary MRI Knee ImagingSoban DaudBelum ada peringkat
- Atlas of Human Anatomy On MRI Spine Extremities Joints PDFDokumen139 halamanAtlas of Human Anatomy On MRI Spine Extremities Joints PDFAnca Mehedintu100% (1)
- Forearm fractures and wrist injuriesDokumen1 halamanForearm fractures and wrist injuriesintan rosliBelum ada peringkat
- Cervical Radiculopathy Clinical PresentationDokumen9 halamanCervical Radiculopathy Clinical PresentationItai IzhakBelum ada peringkat
- Common Spinal Disorders Explained PDFDokumen2 halamanCommon Spinal Disorders Explained PDFTamekaBelum ada peringkat
- Assignments: WHICH TEST? Assignement One: Choose The Appropriate Statistical Test To Address Each of The Following Research QuestionsDokumen3 halamanAssignments: WHICH TEST? Assignement One: Choose The Appropriate Statistical Test To Address Each of The Following Research QuestionsghallabBelum ada peringkat
- Hill - Workshop - Intro To MSK US Shoulder WS 2014-1Dokumen32 halamanHill - Workshop - Intro To MSK US Shoulder WS 2014-1Raihan LuthfiBelum ada peringkat
- Medical Rehabilitation in Compression FractureDokumen32 halamanMedical Rehabilitation in Compression FracturegloriaBelum ada peringkat
- Handout Lat Elbow Pain PDFDokumen47 halamanHandout Lat Elbow Pain PDFgemichan26Belum ada peringkat
- Achilles Tendon RuptureDokumen6 halamanAchilles Tendon RuptureBn Wahyu AjiBelum ada peringkat
- Diagnosis in OrthopaedicsDokumen48 halamanDiagnosis in OrthopaedicsBakta Giri100% (1)
- Patellar InstabilityDokumen16 halamanPatellar InstabilitydrjorgewtorresBelum ada peringkat
- ( ( ( (Dokumen149 halaman( ( ( (Defne Tezel100% (1)
- Simple Guide Orthopadics Chapter 13 Upper Limb ConditionsDokumen20 halamanSimple Guide Orthopadics Chapter 13 Upper Limb ConditionsSurgicalgownBelum ada peringkat
- Elbow WristDokumen59 halamanElbow Wristdr_asalehBelum ada peringkat
- Patterns of Triangular Fibrocartilage Complex (TFCC) Injury Associated WithDokumen7 halamanPatterns of Triangular Fibrocartilage Complex (TFCC) Injury Associated WithCésarLópezBelum ada peringkat
- Diagnosis in Orthopaedic: David Hariadi Masjhoer SMF Orthopedi & Traumatologi RSUD A W SjahranieDokumen24 halamanDiagnosis in Orthopaedic: David Hariadi Masjhoer SMF Orthopedi & Traumatologi RSUD A W SjahranieOkki Masitah Syahfitri NasutionBelum ada peringkat
- Trauma & Orthopaedic SurgeryDokumen120 halamanTrauma & Orthopaedic SurgeryOstazBelum ada peringkat
- Bone Marrow Aspirate Concentrate and Expanded Stem Cell Applications in OrthopaedicsDari EverandBone Marrow Aspirate Concentrate and Expanded Stem Cell Applications in OrthopaedicsBelum ada peringkat
- AGE Advanced Glycation End Products and Diabetic FootDokumen7 halamanAGE Advanced Glycation End Products and Diabetic FootSamBelum ada peringkat
- Surgical Approaches To The Forearm: Robert Strauch MDDokumen18 halamanSurgical Approaches To The Forearm: Robert Strauch MDMichael John TedjajuwanaBelum ada peringkat
- Release Surgery in Stiffness of The KneeDokumen5 halamanRelease Surgery in Stiffness of The KneeMichael John TedjajuwanaBelum ada peringkat
- TENS Surgical TechniqueDokumen32 halamanTENS Surgical TechniqueMichael John TedjajuwanaBelum ada peringkat
- Orthobiologics and Knee Oa PDFDokumen18 halamanOrthobiologics and Knee Oa PDFMichael John TedjajuwanaBelum ada peringkat
- Damage Control Resuscitation in TraumaDokumen8 halamanDamage Control Resuscitation in TraumaMichael John TedjajuwanaBelum ada peringkat
- Damage Control Orthopaedics, Evolving Concepts in The Treatment of Patients Who Have Sustained Orthopaedic TraumaDokumen18 halamanDamage Control Orthopaedics, Evolving Concepts in The Treatment of Patients Who Have Sustained Orthopaedic TraumaMichael John TedjajuwanaBelum ada peringkat
- DiniDokumen10 halamanDiniMuhammad Yasdar BahriBelum ada peringkat
- Orthopaedic Complications of LeprosyDokumen6 halamanOrthopaedic Complications of LeprosyMichael John TedjajuwanaBelum ada peringkat
- 12.posterolateral Approach To Tibial Plafond Fractures A Case SeriesDokumen4 halaman12.posterolateral Approach To Tibial Plafond Fractures A Case SeriesMichael John TedjajuwanaBelum ada peringkat
- Brachial Plexus Injuries in AdultsDokumen10 halamanBrachial Plexus Injuries in AdultsMichael John TedjajuwanaBelum ada peringkat
- Damage Control Orthopaedics, Evolving Concepts in The Treatment of Patients Who Have Sustained Orthopaedic TraumaDokumen18 halamanDamage Control Orthopaedics, Evolving Concepts in The Treatment of Patients Who Have Sustained Orthopaedic TraumaMichael John TedjajuwanaBelum ada peringkat
- Damage Control OrthopaedicsDokumen39 halamanDamage Control OrthopaedicsMichael John TedjajuwanaBelum ada peringkat
- CTEV Parents StoryDokumen6 halamanCTEV Parents StoryMichael John TedjajuwanaBelum ada peringkat
- 01 - History and General Principle of Fracture TreatmentDokumen8 halaman01 - History and General Principle of Fracture TreatmentMichael John TedjajuwanaBelum ada peringkat
- Boutonniere DeformityDokumen24 halamanBoutonniere DeformityMichael John TedjajuwanaBelum ada peringkat
- Guided Growth For The CorrectionDokumen33 halamanGuided Growth For The CorrectionMichael John TedjajuwanaBelum ada peringkat
- Clinical Gait AnalysisDokumen32 halamanClinical Gait AnalysisErem1Belum ada peringkat
- Scoliosis HermanDokumen61 halamanScoliosis HermanMichael John TedjajuwanaBelum ada peringkat
- Pharyngeal ArchDokumen6 halamanPharyngeal ArchRajsandeep SinghBelum ada peringkat
- Trigonum Colli AnteriusDokumen13 halamanTrigonum Colli Anteriusyati rosmiatiBelum ada peringkat
- Colgan 2016Dokumen6 halamanColgan 2016Wahyu InsanBelum ada peringkat
- Splinting InstructionsDokumen19 halamanSplinting Instructionsiris_madrigal100% (1)
- Serratus Anterior Exercises For AbDokumen10 halamanSerratus Anterior Exercises For AbGandhi BabuBelum ada peringkat
- Experimental Evaluation of A Shoulder-Support Exoskeleton For Overhead Work: Influences of Peak Torque Amplitude, Task, and Tool MassDokumen15 halamanExperimental Evaluation of A Shoulder-Support Exoskeleton For Overhead Work: Influences of Peak Torque Amplitude, Task, and Tool MassValentina PetkoffBelum ada peringkat
- Handout Appendicular Skeletal SystemDokumen13 halamanHandout Appendicular Skeletal SystemRhodjane Dela CruzBelum ada peringkat
- Hip Examination - FinalDokumen18 halamanHip Examination - Finalcmonman100% (1)
- MRI of ACLDokumen9 halamanMRI of ACLTri Fara MeliniaBelum ada peringkat
- Muscular SystemDokumen36 halamanMuscular SystemDeepak KdBelum ada peringkat
- ACL InjuryDokumen5 halamanACL InjuryGlen LazarusBelum ada peringkat
- TKA Scope Arthrolysis Knee Surg Sports Traumatol Arthrosc 2010 Mar 18 (3) 346-351Dokumen6 halamanTKA Scope Arthrolysis Knee Surg Sports Traumatol Arthrosc 2010 Mar 18 (3) 346-351Fayza RihastaraBelum ada peringkat
- Dwnload Full Anatomical Basis of Dentistry 3rd Edition Liebgott Test Bank PDFDokumen35 halamanDwnload Full Anatomical Basis of Dentistry 3rd Edition Liebgott Test Bank PDFleo7mco100% (14)
- Lumbar Spine StenosisDokumen12 halamanLumbar Spine StenosisParag DashatwarBelum ada peringkat
- Tripod FractureDokumen45 halamanTripod Fracturekenn ParrochoBelum ada peringkat
- Deformational Plagiocephaly: A Guide To Diagnosis and TreatmentDokumen16 halamanDeformational Plagiocephaly: A Guide To Diagnosis and TreatmentManjunath VaddambalBelum ada peringkat
- Frozen ShoulderDokumen23 halamanFrozen ShoulderpramitaListyBelum ada peringkat
- Lower Limb - CYDokumen9 halamanLower Limb - CYChangYong LeeBelum ada peringkat
- The Lumbar MicrodiscectomyDokumen5 halamanThe Lumbar Microdiscectomyokta fianBelum ada peringkat
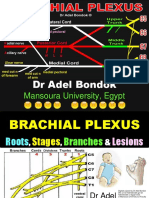
- Brachial Plexus, DR Adel BondokDokumen20 halamanBrachial Plexus, DR Adel BondokSafeBelum ada peringkat
- Musculoskeletal Sports Ultrasound.1Dokumen2 halamanMusculoskeletal Sports Ultrasound.1Mateus AssisBelum ada peringkat
- Osteotomies Jarthrodesis JDokumen41 halamanOsteotomies Jarthrodesis Jdesire kbpBelum ada peringkat
- Symptomatic Valgus Knee - The Surgical OptionsDokumen9 halamanSymptomatic Valgus Knee - The Surgical OptionsSergiu PlescaBelum ada peringkat
- Peripheral Nerves and Plexus. QuestionsDokumen33 halamanPeripheral Nerves and Plexus. QuestionsAmanuelBelum ada peringkat
- Anatomical TermsDokumen8 halamanAnatomical TermsDAGUMAN, FIONA DEI L.Belum ada peringkat