Anda mungkin juga menyukai
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Delhi Factories Rule 1950 PDFDokumen84 halamanDelhi Factories Rule 1950 PDFAkhilesh Kumar SinghBelum ada peringkat
- Oracle Jrockit Mission Control Lab GuideDokumen17 halamanOracle Jrockit Mission Control Lab GuideashuhegdeBelum ada peringkat
- FR-8x Editor Eng01 WDokumen8 halamanFR-8x Editor Eng01 WRadulian Daniel100% (1)
- 1998-10 The Computer Paper - Ontario EditionDokumen156 halaman1998-10 The Computer Paper - Ontario Editionthecomputerpaper100% (1)
- TDS Sadechaf UVACRYL 2151 - v9Dokumen5 halamanTDS Sadechaf UVACRYL 2151 - v9Alex MacabuBelum ada peringkat
- Gathering Network RequirementsDokumen30 halamanGathering Network RequirementsAmin ZangetsuBelum ada peringkat
- Chapter 19A ConcreteDokumen10 halamanChapter 19A ConcreteMofasa EBelum ada peringkat
- Materials Today: Proceedings: Avula Suresh, T. Nancharaiah, Ravikumar Dumpala, B. Ratna SunilDokumen5 halamanMaterials Today: Proceedings: Avula Suresh, T. Nancharaiah, Ravikumar Dumpala, B. Ratna SunilBart MaxBelum ada peringkat
- BKLT DeaeratorDokumen24 halamanBKLT Deaeratormalikgaurav01Belum ada peringkat
- Water Treatment Process Disinfection PDFDokumen6 halamanWater Treatment Process Disinfection PDFAriff JasniBelum ada peringkat
- Component Modeling - HDokumen5 halamanComponent Modeling - HVasu IyerBelum ada peringkat
- EN 1991-1-4 NA enDokumen4 halamanEN 1991-1-4 NA enanuj3936100% (1)
- SinxbyxDokumen9 halamanSinxbyxGreeshmaBelum ada peringkat
- NBN Co: Financial Management SolutionDokumen2 halamanNBN Co: Financial Management SolutionAccentureAustraliaBelum ada peringkat
- PIONEER AUTORADIO Deh-X4850bt Deh-X6850bt Operating Manual Ing - Esp - PorDokumen72 halamanPIONEER AUTORADIO Deh-X4850bt Deh-X6850bt Operating Manual Ing - Esp - PorJesus NinalayaBelum ada peringkat
- Applying Six Sigma at 3MDokumen13 halamanApplying Six Sigma at 3MdchBelum ada peringkat
- Q3 NSP - SLP - RLPDokumen41 halamanQ3 NSP - SLP - RLPRushi RavalBelum ada peringkat
- PT14 Engine Monitor 1Dokumen2 halamanPT14 Engine Monitor 1BJ DixBelum ada peringkat
- An Introduction Into The Feynman Path Integral PDFDokumen94 halamanAn Introduction Into The Feynman Path Integral PDFLivardy WufiantoBelum ada peringkat
- Bubbling Kun NiDokumen7 halamanBubbling Kun NiBelen CRBelum ada peringkat
- Comfort and Performance Your Customers DemandDokumen18 halamanComfort and Performance Your Customers Demandgizex2013Belum ada peringkat
- RT 8090 TDokumen40 halamanRT 8090 TManuel100% (1)
- Ibr CalculationsDokumen9 halamanIbr Calculationsaroonchelikani67% (3)
- Restoration and Adaptive Re-Use of Queen Mary's High School: Phase-1Dokumen4 halamanRestoration and Adaptive Re-Use of Queen Mary's High School: Phase-1Sonali GurungBelum ada peringkat
- Tube Well Design Project SolutionDokumen5 halamanTube Well Design Project SolutionEng Ahmed abdilahi IsmailBelum ada peringkat
- Philips Aquatrio FC7070 - 01 Esploso ManualeDokumen9 halamanPhilips Aquatrio FC7070 - 01 Esploso ManualeRocco Mangione0% (1)
- Doing Hot Work On Gas ShipDokumen5 halamanDoing Hot Work On Gas ShipAnonymous icnhaNsFBelum ada peringkat
- Slope Stability in Slightly Fissured Claystones and MarlsDokumen25 halamanSlope Stability in Slightly Fissured Claystones and MarlsrullyirwandiBelum ada peringkat
- VLE Lactic Acid Ethyl Lactate Esterification PDFDokumen7 halamanVLE Lactic Acid Ethyl Lactate Esterification PDFAseem Kashyap0% (1)
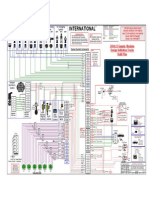
- Esquema Elétrico NGD 9.3Dokumen2 halamanEsquema Elétrico NGD 9.3LuisCarlosKovalchuk100% (1)