Anda mungkin juga menyukai
- NutrisiEnteralHCUDokumen4 halamanNutrisiEnteralHCUTias DiahBelum ada peringkat
- WarfarinDokumen18 halamanWarfarinMuhammad Sandy IrwansyahBelum ada peringkat
- Hepatitis MarkerDokumen19 halamanHepatitis MarkerSiti Hardianti Mahlan100% (2)
- Komplikasi Transfusi Darah: Diagnosis, Pengobatan, dan PencegahanDokumen44 halamanKomplikasi Transfusi Darah: Diagnosis, Pengobatan, dan PencegahanasriBelum ada peringkat
- DETEKSI DINI PENYAKIT PARUDokumen22 halamanDETEKSI DINI PENYAKIT PARUdea sandra prastyscilyaBelum ada peringkat
- URINALISIS DAN CAMPURAN TUBUHDokumen173 halamanURINALISIS DAN CAMPURAN TUBUHDikin DBelum ada peringkat
- NCPH Dan IphDokumen7 halamanNCPH Dan IphBelinda HartoBelum ada peringkat
- Kelainan TiroidDokumen61 halamanKelainan TiroidRiezca DeviBelum ada peringkat
- Catatan (BONE MARROW ASPIRATION)Dokumen5 halamanCatatan (BONE MARROW ASPIRATION)El ElBelum ada peringkat
- HiperbilirubinemiaDokumen50 halamanHiperbilirubinemiaYeyen NadianBelum ada peringkat
- Bab Ii Kajian PustakaDokumen30 halamanBab Ii Kajian PustakaAmboy YallyBelum ada peringkat
- Adenosine DeaminaseDokumen2 halamanAdenosine Deaminaseerna100% (1)
- Patogenesis Adenotonsilitis Kronis + OSASDokumen5 halamanPatogenesis Adenotonsilitis Kronis + OSASBenne Lauda AnnanditaBelum ada peringkat
- 2 2 1 5 PDFDokumen17 halaman2 2 1 5 PDFAdrian ArdimayBelum ada peringkat
- ENDOCARDITISDokumen35 halamanENDOCARDITISSri MulianiBelum ada peringkat
- ASUHAN KEPERAWATAN PADA PASIEN THALASSEMIADokumen26 halamanASUHAN KEPERAWATAN PADA PASIEN THALASSEMIAShilny MBelum ada peringkat
- DBD Pemeriksaan Laboratorium dan TatalaksanaDokumen4 halamanDBD Pemeriksaan Laboratorium dan TatalaksanadodikBelum ada peringkat
- Cairan PleuraDokumen13 halamanCairan PleuraYasmin AlqadriBelum ada peringkat
- Update On Massive Transfusion-BJA 2013Dokumen71 halamanUpdate On Massive Transfusion-BJA 2013Yuritsa LeonardBelum ada peringkat
- Anatomi PleuraDokumen86 halamanAnatomi PleuraFebrina SintariBelum ada peringkat
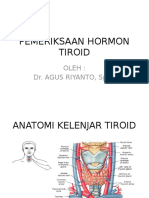
- Pemeriksaan Hormon TiroidDokumen18 halamanPemeriksaan Hormon TiroidOkti Dewi ChaidirBelum ada peringkat
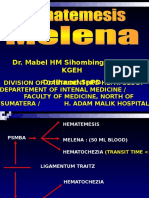
- HEMATEMESISDokumen37 halamanHEMATEMESISM Effendy Nugraha HasibuanBelum ada peringkat
- Cidera Kepala TatalaksanaDokumen2 halamanCidera Kepala Tatalaksanabagus wandaBelum ada peringkat
- Ebstein's Anomaly Referat Cardio Pedi Azizi BTKVDokumen25 halamanEbstein's Anomaly Referat Cardio Pedi Azizi BTKVAzizi PranokoBelum ada peringkat
- Pemeriksaan Lab PD TrombosisDokumen36 halamanPemeriksaan Lab PD Trombosisluthfi_ramdhaniBelum ada peringkat
- CSS Seromarker HepatitisDokumen15 halamanCSS Seromarker HepatitisMohamad Asyraf Mohd RoslyBelum ada peringkat
- Algoritma NICEDokumen3 halamanAlgoritma NICEAdhella Menur NaysillaBelum ada peringkat
- Skills Lab 4 - Anamnesis (Hematologi)Dokumen3 halamanSkills Lab 4 - Anamnesis (Hematologi)Rici Pernando SihombingBelum ada peringkat
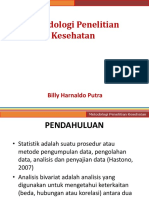
- Metodologi Penelitian KesehatanDokumen54 halamanMetodologi Penelitian KesehatanceciliaBelum ada peringkat
- Transudat & EksudatDokumen16 halamanTransudat & EksudatTsintani Nur AristianaBelum ada peringkat
- Laporan Kasus PnaDokumen11 halamanLaporan Kasus PnaKevinBelum ada peringkat
- Washed Red CellDokumen3 halamanWashed Red Cellera anggoro kusuma ningrum100% (1)
- Obat DigitalisDokumen1 halamanObat Digitaliskyumir100% (1)
- HF+OMI+AF+LVThrombusDokumen36 halamanHF+OMI+AF+LVThrombusLaily AgustinaBelum ada peringkat
- Trichomonas VaginalisDokumen5 halamanTrichomonas VaginalisArya DharmikaBelum ada peringkat
- Manifestasi Klinis Leptospirosis, Malaria, HepatititsDokumen5 halamanManifestasi Klinis Leptospirosis, Malaria, HepatititsIntan KarmilaBelum ada peringkat
- Anatomi Dan Fisiologi PleuraDokumen2 halamanAnatomi Dan Fisiologi PleuraNida KhofiaBelum ada peringkat
- Catatan Bedah AnakDokumen17 halamanCatatan Bedah AnakrynaldiandriansyaBelum ada peringkat
- Lapkas IBDDokumen35 halamanLapkas IBDkarin100% (1)
- ThalasemiaDokumen16 halamanThalasemiaDavid SilalahiBelum ada peringkat
- DARAHDokumen41 halamanDARAHStephanie NieBelum ada peringkat
- Mycobacterium Other Than Tuberculosis (MOTT)Dokumen28 halamanMycobacterium Other Than Tuberculosis (MOTT)nurul aliyahBelum ada peringkat
- Tugas 1Dokumen25 halamanTugas 1Syahrul AdzimBelum ada peringkat
- Golongan Darah ABODokumen14 halamanGolongan Darah ABOReza Angga PratamaBelum ada peringkat
- Pengendalian PendarahanDokumen23 halamanPengendalian PendarahanRahmani Scout MovemenBelum ada peringkat
- Referat DengueDokumen48 halamanReferat DengueAnnisa Nur MaulidyaBelum ada peringkat
- Upl Patofisiologi C AsitesDokumen20 halamanUpl Patofisiologi C AsitesChrsytanti Melissa MelatiBelum ada peringkat
- Crs Dindar PPT DBD KDKDokumen53 halamanCrs Dindar PPT DBD KDKdokterbotakBelum ada peringkat
- KolesistitisDokumen4 halamanKolesistitisHaruno RosydzBelum ada peringkat
- KP 36 Temuan Otopsi Pada Sudden Cardiac DeathDokumen36 halamanKP 36 Temuan Otopsi Pada Sudden Cardiac DeathHasraMukhlisanBelum ada peringkat
- Efusi Pleura PenangananDokumen11 halamanEfusi Pleura PenangananYusrina Nur RahmaBelum ada peringkat
- Atrial FlutterDokumen19 halamanAtrial FlutterArfan Arrasyid100% (1)
- LAPORAN MEDIS PASIENDokumen84 halamanLAPORAN MEDIS PASIENVania Eka PutriBelum ada peringkat
- Lapkas HemotoraksDokumen26 halamanLapkas HemotoraksJohanes NadapdapBelum ada peringkat
- Referat Cairan Serebrospinal FixDokumen43 halamanReferat Cairan Serebrospinal FixDear Farah SielmaBelum ada peringkat
- Transfusi DarahDokumen28 halamanTransfusi DarahwelBelum ada peringkat
- Transfusi DarahDokumen32 halamanTransfusi Darahwinda2667% (3)
- Transfusi DarahDokumen42 halamanTransfusi DarahRirin AgustinBelum ada peringkat
- Transfusi Darah IpdDokumen42 halamanTransfusi Darah IpdRusdin Ode JaeBelum ada peringkat
- TRANSFUSI DARAHDokumen41 halamanTRANSFUSI DARAHaldwint09Belum ada peringkat
- STEREOKIMIA DAN RESONANSIDokumen42 halamanSTEREOKIMIA DAN RESONANSIGilang Adi NugrahaBelum ada peringkat
- Lowongan-Konsultan-Sarana-Dan-Prasarana 20120223105125 0Dokumen2 halamanLowongan-Konsultan-Sarana-Dan-Prasarana 20120223105125 0Gilang Adi NugrahaBelum ada peringkat
- Chapter IIDokumen11 halamanChapter IIRakhmat24Belum ada peringkat
- 70 204 1 PB113 120Dokumen8 halaman70 204 1 PB113 120Gilang Adi NugrahaBelum ada peringkat
- Efek Fotokatalisis Nano TiO2Dokumen69 halamanEfek Fotokatalisis Nano TiO2Gilang Adi NugrahaBelum ada peringkat
- BAB II Tinjauan PustakaDokumen7 halamanBAB II Tinjauan PustakaSyarfan Maulana RahmanBelum ada peringkat
- Pengantar StatistikDokumen5 halamanPengantar StatistikBintoro Wicaksono SunyotoBelum ada peringkat
- Karbon Aktif Dan Tio2Dokumen5 halamanKarbon Aktif Dan Tio2Gilang Adi NugrahaBelum ada peringkat
- Kimia Silikat dan SilikaDokumen14 halamanKimia Silikat dan SilikaGilang Adi Nugraha100% (1)
- Kimia Organik IDokumen222 halamanKimia Organik IAprilianti Dwi Fitria Faisal67% (3)
- Makalah04 Volume 29 No 2 2011Dokumen10 halamanMakalah04 Volume 29 No 2 2011Devi YunitaBelum ada peringkat
- Atmosfer Dan Kimia AtmosferDokumen38 halamanAtmosfer Dan Kimia AtmosferGilang Adi NugrahaBelum ada peringkat
- Makalah FotosintesisDokumen11 halamanMakalah FotosintesisNovitaBelum ada peringkat
- Pengantar StatistikDokumen5 halamanPengantar StatistikBintoro Wicaksono SunyotoBelum ada peringkat
- STEREOKIMIA DAN RESONANSIDokumen42 halamanSTEREOKIMIA DAN RESONANSIGilang Adi NugrahaBelum ada peringkat
- ANALISIS KADAR β-KAROTEN PADA BUAH PAREDokumen25 halamanANALISIS KADAR β-KAROTEN PADA BUAH PAREGilang Adi NugrahaBelum ada peringkat
- Tugas SilicaDokumen14 halamanTugas SilicaGilang Adi NugrahaBelum ada peringkat
- Tugas Kimling 1Dokumen3 halamanTugas Kimling 1Gilang Adi NugrahaBelum ada peringkat
- Spektrofotometri UvDokumen3 halamanSpektrofotometri UvGilang Adi NugrahaBelum ada peringkat
- Tugas WirusDokumen1 halamanTugas WirusGilang Adi NugrahaBelum ada peringkat
- Tugas LitKimDokumen3 halamanTugas LitKimGilang Adi NugrahaBelum ada peringkat
- 5 MANFAAT DONOR DARAHDokumen2 halaman5 MANFAAT DONOR DARAHGilang Adi NugrahaBelum ada peringkat
- 457 698 1 SMDokumen4 halaman457 698 1 SMevin34100% (1)
- Tugas LitKimDokumen3 halamanTugas LitKimGilang Adi NugrahaBelum ada peringkat
- Zat Warna Kelompok 4Dokumen18 halamanZat Warna Kelompok 4Gilang Adi NugrahaBelum ada peringkat
- Zat Warna Kelompok 4Dokumen18 halamanZat Warna Kelompok 4Gilang Adi NugrahaBelum ada peringkat
- Spektrofotometri UvDokumen3 halamanSpektrofotometri UvGilang Adi NugrahaBelum ada peringkat
- KUTU PENYAKITDokumen5 halamanKUTU PENYAKITGilang Adi NugrahaBelum ada peringkat
- 5 MANFAAT DONOR DARAHDokumen2 halaman5 MANFAAT DONOR DARAHGilang Adi NugrahaBelum ada peringkat