Anda mungkin juga menyukai
- Ob Gyn Sample HisotryDokumen4 halamanOb Gyn Sample HisotrySophia RubiaBelum ada peringkat
- GyneDokumen88 halamanGyneSamiti HjBelum ada peringkat
- Hiv in Pregnancy FinalDokumen22 halamanHiv in Pregnancy FinalMoin PandithBelum ada peringkat
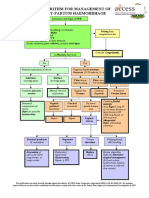
- 15 NG - PPH Algorithm-Aug08Dokumen2 halaman15 NG - PPH Algorithm-Aug08abdelhamed aliBelum ada peringkat
- GLM0021 Postpartum Haemorrhage PDFDokumen15 halamanGLM0021 Postpartum Haemorrhage PDFRubiahSheBiachBelum ada peringkat
- Ob CPCDokumen80 halamanOb CPCDonna Meryll Eduave-EsguerraBelum ada peringkat
- History & Physical Exam in Ob/Gyn: By: - DR AmanuDokumen75 halamanHistory & Physical Exam in Ob/Gyn: By: - DR AmanuKåbåñå TürüñåBelum ada peringkat
- Obstetrics - Abnormalities of The Amniotic FluidDokumen6 halamanObstetrics - Abnormalities of The Amniotic FluidJonathanBelum ada peringkat
- Obstructed LabourDokumen2 halamanObstructed LabourAvinash BarhateBelum ada peringkat
- Ob SGDDokumen88 halamanOb SGDFerdinand Luis SuarezBelum ada peringkat
- Case History Ob & Gyne 4Dokumen6 halamanCase History Ob & Gyne 4maksventileBelum ada peringkat
- Complaints ScenariosDokumen8 halamanComplaints ScenariosJaypee Fabros EdraBelum ada peringkat
- History Examination of Gynecology and Obstetrics PatientsDokumen3 halamanHistory Examination of Gynecology and Obstetrics PatientsAgus WijayaBelum ada peringkat
- GRP II Gyne CaseDokumen72 halamanGRP II Gyne CaseGreggy John Rivera CascayanBelum ada peringkat
- Normal Conduct of LaborDokumen62 halamanNormal Conduct of LaborFaye Cabotaje LinganBelum ada peringkat
- Placenta PreviaDokumen36 halamanPlacenta Previaotartil_nimanBelum ada peringkat
- 24 HR History 2Dokumen2 halaman24 HR History 2Arjun KatariaBelum ada peringkat
- Breech Presentation: Penny Lyne Jalius Group 4 4 Year 1 Semester 2011Dokumen23 halamanBreech Presentation: Penny Lyne Jalius Group 4 4 Year 1 Semester 2011Penny Julius R MirohBelum ada peringkat
- 1st Cwu OngDokumen18 halaman1st Cwu Ongdila_ayubBelum ada peringkat
- Multinodular Goitre Case PresentationDokumen19 halamanMultinodular Goitre Case PresentationTamilBelum ada peringkat
- Pedia HX Seizure 1Dokumen25 halamanPedia HX Seizure 1Amer Hussein DomadoBelum ada peringkat
- Obstetrics Case PresentationDokumen27 halamanObstetrics Case PresentationMahaprasad sahoo 77Belum ada peringkat
- Cerebral PalsyDokumen14 halamanCerebral PalsyWaode SittrisnawatiBelum ada peringkat
- Case Discussion-FibroidDokumen17 halamanCase Discussion-FibroidNazee NazreenBelum ada peringkat
- Case 01 - Maternal PhysiologyDokumen5 halamanCase 01 - Maternal PhysiologyRem AlfelorBelum ada peringkat
- Pediatric Urinary Tract Infection Case StudyDokumen17 halamanPediatric Urinary Tract Infection Case StudyKyla Barrera TabungarBelum ada peringkat
- History Taking OBS GYNDokumen10 halamanHistory Taking OBS GYNzvkznhsw2tBelum ada peringkat
- Case 1 History & PEDokumen3 halamanCase 1 History & PEcbac1990Belum ada peringkat
- Treatment of Fistula in AnoDokumen30 halamanTreatment of Fistula in Ano09172216507Belum ada peringkat
- Specimen Case Presentation Write-Up Obstetrics Case SummaryDokumen9 halamanSpecimen Case Presentation Write-Up Obstetrics Case SummaryAngeline RodriguesBelum ada peringkat
- BY: Shazlin Bt. Sabaah Salwa Hanim Bt. Mohd. Saifuddin Kamarulzaman B. MuzainiDokumen61 halamanBY: Shazlin Bt. Sabaah Salwa Hanim Bt. Mohd. Saifuddin Kamarulzaman B. MuzainiJohn Christopher LucesBelum ada peringkat
- Small Group DiscussionDokumen3 halamanSmall Group DiscussionBea SamonteBelum ada peringkat
- GYNE UltrasoundgyneDokumen11 halamanGYNE UltrasoundgyneMara AbantoBelum ada peringkat
- O and G Notes Notebank NumberedDokumen173 halamanO and G Notes Notebank NumberedPerscitus Ali القحطانيBelum ada peringkat
- Group II Makati Medical Center m8 1Dokumen107 halamanGroup II Makati Medical Center m8 1CASSANDRAJUL VARINBelum ada peringkat
- CC C C: June 8, 2011 By: Santos, Edilberto DBDokumen63 halamanCC C C: June 8, 2011 By: Santos, Edilberto DBHakugeiBelum ada peringkat
- Amenore Galactorea, Hyperprolactinemia, Adenoma Hypophysis DR M Yusuf SpOGDokumen24 halamanAmenore Galactorea, Hyperprolactinemia, Adenoma Hypophysis DR M Yusuf SpOGPuji Yunisyah RahayuBelum ada peringkat
- Case Protocol OB - H MOLEDokumen3 halamanCase Protocol OB - H MOLEKim Adarem Joy ManimtimBelum ada peringkat
- Fistula in AnoDokumen4 halamanFistula in AnoosamabinziaBelum ada peringkat
- 107 Rle Virtual Duty - Opd: Internal MedicineDokumen6 halaman107 Rle Virtual Duty - Opd: Internal MedicineGiel Margareth LindoBelum ada peringkat
- Case Title: PreeclampsiaDokumen6 halamanCase Title: PreeclampsiaLanaBelum ada peringkat
- Clinical Findings: ACOG - Cervical Insufficiency As "Dokumen5 halamanClinical Findings: ACOG - Cervical Insufficiency As "lllBelum ada peringkat
- HTN Complicating PregnancyDokumen18 halamanHTN Complicating PregnancyAiman ArifinBelum ada peringkat
- The Medical Management of Abnormal Uterine Bleeding in Reproductive-Aged WomenDokumen14 halamanThe Medical Management of Abnormal Uterine Bleeding in Reproductive-Aged Womendiegoesteban1234Belum ada peringkat
- 002 Intrapartum Fetal Heart Rate Monitoring 3a - ACOG Bulletin 106 PDFDokumen11 halaman002 Intrapartum Fetal Heart Rate Monitoring 3a - ACOG Bulletin 106 PDFale_fearBelum ada peringkat
- Correlative AnatomyDokumen19 halamanCorrelative AnatomyLicensed to HealBelum ada peringkat
- Case Report MartaDokumen10 halamanCase Report MartadenekeBelum ada peringkat
- Recent Advances in Gynaec UsgDokumen46 halamanRecent Advances in Gynaec UsgKalpavriksha1974Belum ada peringkat
- OBGYN Objective - Module Study GuideDokumen79 halamanOBGYN Objective - Module Study GuideHema LaughsalotBelum ada peringkat
- Joint Pain - ApproachDokumen32 halamanJoint Pain - ApproachHassan Bin AjmalBelum ada peringkat
- Menstrual Cycle Made SimpleDokumen6 halamanMenstrual Cycle Made SimpleNurul Nabilah AzraBelum ada peringkat
- Cervical Insufficiency:: Miscarriage Early (Premature)Dokumen2 halamanCervical Insufficiency:: Miscarriage Early (Premature)Ardelean EmanuelBelum ada peringkat
- Peads NotesDokumen18 halamanPeads Notesechofox11Belum ada peringkat
- PartogramDokumen31 halamanPartogramRemelou Garchitorena AlfelorBelum ada peringkat
- Ob-Gyn Review Part 3Dokumen101 halamanOb-Gyn Review Part 3filchibuffBelum ada peringkat
- Precocious VS Early Puberty, SiskaDokumen21 halamanPrecocious VS Early Puberty, SiskapuspaBelum ada peringkat
- Surgery 2 Case ReportDokumen12 halamanSurgery 2 Case ReportElvis NgBelum ada peringkat
- Case No: Ectopic PregnancyDokumen15 halamanCase No: Ectopic PregnancydellaBelum ada peringkat
- Case Report NODokumen22 halamanCase Report NOcuepBelum ada peringkat
- 106, Mrs T 36 Hydatiform MoleDokumen16 halaman106, Mrs T 36 Hydatiform MoleShawn DyerBelum ada peringkat
- Uterine Myoma in Depth Case Study For MAN-MSDokumen88 halamanUterine Myoma in Depth Case Study For MAN-MSJacyn Mae S. RefamonteBelum ada peringkat
- Fundamentals of Stroke and TIADokumen12 halamanFundamentals of Stroke and TIAMaria WibawaBelum ada peringkat
- MaryDokumen4 halamanMaryAnonymous oQvrJSxBelum ada peringkat
- BreechDokumen2 halamanBreechBrel KirbyBelum ada peringkat
- NCM 109 Prelims ReviewerDokumen2 halamanNCM 109 Prelims ReviewerReyna Chame GarcinezBelum ada peringkat
- Pembimbing: Dr. Refni Muslim SP.R (K) Presenter: Dr. Ardyanto FlorensiusDokumen34 halamanPembimbing: Dr. Refni Muslim SP.R (K) Presenter: Dr. Ardyanto FlorensiusBeatrice Cynthia WalterBelum ada peringkat
- Bleeding in PregnancyDokumen24 halamanBleeding in PregnancyReznitha AkhmadBelum ada peringkat
- SDO - TARLAC CITY - MABALACAT - CSE MODULE - HUMAN AND BODY DEVELOPMENT For 4th 2Dokumen28 halamanSDO - TARLAC CITY - MABALACAT - CSE MODULE - HUMAN AND BODY DEVELOPMENT For 4th 2Ma Concepcion Adriano GuansingBelum ada peringkat
- Catherine M. Metra BSN IvDokumen18 halamanCatherine M. Metra BSN IvCatherine MetraBelum ada peringkat
- Skenario C Blok 22Dokumen40 halamanSkenario C Blok 22Ambhi GanaBelum ada peringkat
- Female Reproductive SystemDokumen7 halamanFemale Reproductive Systemkristel ludangcoBelum ada peringkat
- Augmenting Cervimetry, Fetal Survivability, Calving Ease, and Uterine Health During Buffalo Uterine Torsion TreatmentDokumen12 halamanAugmenting Cervimetry, Fetal Survivability, Calving Ease, and Uterine Health During Buffalo Uterine Torsion TreatmentIJAR JOURNALBelum ada peringkat
- Surgical Cs Case Study - BangDokumen25 halamanSurgical Cs Case Study - BangClyde R.OrtegaBelum ada peringkat
- Davinci Medical AcademyDokumen26 halamanDavinci Medical Academysk100% (2)
- Drug Study: College of NursingDokumen14 halamanDrug Study: College of NursingelleBelum ada peringkat
- Maternal Physiology 25th OB WilliamsDokumen62 halamanMaternal Physiology 25th OB WilliamsDee SarajanBelum ada peringkat
- CCS 010 - HIV, AIDS - Class VER - SEPT 2010 (Autosaved)Dokumen46 halamanCCS 010 - HIV, AIDS - Class VER - SEPT 2010 (Autosaved)Betty SymonBelum ada peringkat
- Metritis and PyometraDokumen7 halamanMetritis and PyometraGonzález Mendoza DamielBelum ada peringkat
- Abnormal Progress in Labor (Precipitous Labor and Birth & Retraction Rings)Dokumen34 halamanAbnormal Progress in Labor (Precipitous Labor and Birth & Retraction Rings)Ana100% (3)
- Abdomen - Pelvis: Lecturer: Prof. Dr. Wahyuni Lukita Atmodjo, PH.DDokumen33 halamanAbdomen - Pelvis: Lecturer: Prof. Dr. Wahyuni Lukita Atmodjo, PH.DAgatha FeliciaBelum ada peringkat
- The Sexual SelfDokumen30 halamanThe Sexual SelfGilbert BelmisBelum ada peringkat
- Uterine Fibroids Case StudyDokumen38 halamanUterine Fibroids Case StudyFiona Cheryl Amsterdam80% (5)
- 107 Lec Finals 3RD LessonDokumen8 halaman107 Lec Finals 3RD LessonChona CastorBelum ada peringkat
- High Risk Pregnancy:: A Woman Who Develops A Complication of PregnancyDokumen79 halamanHigh Risk Pregnancy:: A Woman Who Develops A Complication of PregnancyMike Faustino SolangonBelum ada peringkat
- The Fertility Cleanse Guide Ebook1Dokumen19 halamanThe Fertility Cleanse Guide Ebook1Laura BarriosBelum ada peringkat
- Medical Terminology Reproductive SystemDokumen130 halamanMedical Terminology Reproductive SystemsheshBelum ada peringkat
- 17 11 16 Puerperial SepsisDokumen15 halaman17 11 16 Puerperial SepsisJerry MwandoroBelum ada peringkat
- Urogenital SystemDokumen111 halamanUrogenital Systemhamdan hamimBelum ada peringkat
- Jurnal Helpi Nelwatri 2015Dokumen5 halamanJurnal Helpi Nelwatri 2015rani arvitaBelum ada peringkat
- 2016 Book CongenitalMüllerianAnomaliesDokumen151 halaman2016 Book CongenitalMüllerianAnomaliesQui Nguyen MinhBelum ada peringkat