Anda mungkin juga menyukai
- Pressure Ulcer Prevention and TreatmentDokumen51 halamanPressure Ulcer Prevention and TreatmentIosefina DudeanuBelum ada peringkat
- Uint No 6 Skin IntegretyDokumen23 halamanUint No 6 Skin Integretyeshasohaib92Belum ada peringkat
- Pressure Ulcers: Francisco Torres Lozada MD Ponce Health Sciences University GeriatricsDokumen67 halamanPressure Ulcers: Francisco Torres Lozada MD Ponce Health Sciences University GeriatricsStephanie RiveraBelum ada peringkat
- Skin Care PowerpointDokumen52 halamanSkin Care Powerpointisapatrick812667% (3)
- Assessing and Classifying Pressure SoresDokumen7 halamanAssessing and Classifying Pressure SoresAnnette Baines100% (1)
- Pressure Sores & ManagementDokumen15 halamanPressure Sores & Managementmupt77Belum ada peringkat
- 2 Skin-IntegrityDokumen74 halaman2 Skin-IntegrityFlourence ZafranBelum ada peringkat
- Wound AssessmentDokumen4 halamanWound Assessmentonlyabc123Belum ada peringkat
- Pressure Ulcers Hand OutDokumen52 halamanPressure Ulcers Hand OutAdiAri RosiuBelum ada peringkat
- Unit 11 Skin Integrity and Wound CareDokumen47 halamanUnit 11 Skin Integrity and Wound CareAshaBelum ada peringkat
- RNSG 1413wounds Fall2006Dokumen67 halamanRNSG 1413wounds Fall2006api-3697326100% (1)
- What Is Pressure Ulcer?: Signs and SymptomsDokumen6 halamanWhat Is Pressure Ulcer?: Signs and Symptomsshenecajean carajayBelum ada peringkat
- Wound CareDokumen10 halamanWound CareKenima Idao100% (3)
- Decubitus UlcerDokumen30 halamanDecubitus UlcerZgama AbdulrahmanBelum ada peringkat
- WOUND CARE and BANDAGINGDokumen9 halamanWOUND CARE and BANDAGINGJane BelvisBelum ada peringkat
- S M D U: KIN Anagement Ecubitis LcerDokumen77 halamanS M D U: KIN Anagement Ecubitis LcerabidBelum ada peringkat
- Wound CareDokumen7 halamanWound CareAbogadie Dione Blas ReyBelum ada peringkat
- Perawatan LukaDokumen54 halamanPerawatan LukaLa Fith MbozoBelum ada peringkat
- Decubitus UlcerDokumen14 halamanDecubitus Ulcerayman100% (3)
- Wound CareDokumen77 halamanWound CareNestor Balboa100% (1)
- Pressure Ulcers- Surgery i March 2019Dokumen63 halamanPressure Ulcers- Surgery i March 2019daniyfondoBelum ada peringkat
- Decubitus UlcerDokumen8 halamanDecubitus UlcerDanilo EspinoBelum ada peringkat
- BASIC WOUND CARE GUIDEDokumen30 halamanBASIC WOUND CARE GUIDEHysainth DescalzotaBelum ada peringkat
- Tissue Integrity Outline Spring 2023Dokumen25 halamanTissue Integrity Outline Spring 2023morganstorey0Belum ada peringkat
- Pressure Ulcer Care Guide: Stages, Treatments & Nursing InterventionsDokumen39 halamanPressure Ulcer Care Guide: Stages, Treatments & Nursing InterventionsRosalyn YuBelum ada peringkat
- Pressure UlcersDokumen38 halamanPressure UlcersRadwa EbedBelum ada peringkat
- Pressure UlcerDokumen66 halamanPressure UlcerSwarnkar JayeshBelum ada peringkat
- Pressure Ulcers: Jorge G. Ruiz, MD, FACPDokumen71 halamanPressure Ulcers: Jorge G. Ruiz, MD, FACPRomilPatelBelum ada peringkat
- Skin Injury: Dr. Imam FirmansyahDokumen28 halamanSkin Injury: Dr. Imam FirmansyahVanquish VeinBelum ada peringkat
- Skin Integrity Epidermis-Multiple Layers, Stratum Corneum - ThinDokumen11 halamanSkin Integrity Epidermis-Multiple Layers, Stratum Corneum - ThinsakonzBelum ada peringkat
- Types of Wounds and Phases of HealingDokumen6 halamanTypes of Wounds and Phases of HealingAsniah Hadjiadatu AbdullahBelum ada peringkat
- Unit # 06 Skin Management Insta Husain.z.kmuDokumen43 halamanUnit # 06 Skin Management Insta Husain.z.kmuAamir IqbalBelum ada peringkat
- Hips Back Ankles Buttocks HeelsDokumen13 halamanHips Back Ankles Buttocks Heelsفرزدق الحسيناويBelum ada peringkat
- Pressure SoresDokumen20 halamanPressure SoresRupika Sodhi100% (1)
- Wound Care Gopi SirDokumen110 halamanWound Care Gopi SirArvind ShenoyBelum ada peringkat
- Assessing and Preventing Pressure UlcersDokumen8 halamanAssessing and Preventing Pressure UlcersTamil VillardoBelum ada peringkat
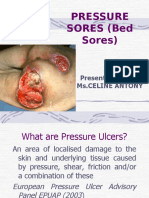
- Pressure Sores (Bed Sores) : Presented By: Ms - Celine AntonyDokumen40 halamanPressure Sores (Bed Sores) : Presented By: Ms - Celine AntonyjyothiBelum ada peringkat
- Chapter 48 - Skin Integrity and Wound CareDokumen13 halamanChapter 48 - Skin Integrity and Wound CareHaji Raji100% (1)
- Skin Integrity and Wound Care: Types, Stages, and Risk FactorsDokumen25 halamanSkin Integrity and Wound Care: Types, Stages, and Risk FactorsMitul PeterBelum ada peringkat
- Bed SoresDokumen15 halamanBed Soresver_at_work100% (1)
- Pressure Sore Prevention & TreatmentDokumen21 halamanPressure Sore Prevention & TreatmentDrsauga France100% (1)
- Skin IntegrityDokumen56 halamanSkin IntegrityneehoshiBelum ada peringkat
- 4.wound Care IDokumen46 halaman4.wound Care Iamir aizatBelum ada peringkat
- Fundamentals of Nursing: Skin Integrity and Wound CareDokumen32 halamanFundamentals of Nursing: Skin Integrity and Wound CareFEVIE ANNE BANATAOBelum ada peringkat
- The Skin Is An Organ of ProtectionDokumen5 halamanThe Skin Is An Organ of ProtectionFahmi Sulistyo HutomoBelum ada peringkat
- Wound Care 1Dokumen12 halamanWound Care 1Afril CadagBelum ada peringkat
- Wound Management GuidelinesDokumen12 halamanWound Management GuidelinesFransiscus Braveno RapaBelum ada peringkat
- Skin Management Decubitis Ulcer: Presented By: Maj (R) Nazma Noreen N/Lecturer ION/WMC Wah CanttDokumen77 halamanSkin Management Decubitis Ulcer: Presented By: Maj (R) Nazma Noreen N/Lecturer ION/WMC Wah CanttabidBelum ada peringkat
- 4 Wounds and Wound CareDokumen25 halaman4 Wounds and Wound Caredoc-fahad aftabBelum ada peringkat
- 2 - Wounds, Tissue Repair and ScaresDokumen26 halaman2 - Wounds, Tissue Repair and Scaresnightfury200313Belum ada peringkat
- Pathophysiology and Prevention of Scar Tissues - NataDokumen45 halamanPathophysiology and Prevention of Scar Tissues - Natadenybudiman04100% (1)
- Wound ClassificationDokumen48 halamanWound Classificationzarizi100% (2)
- Wound Assessment: Pusat Perawatan Luka "Patria Care" Stikes Patria Husada BLITAR 2019Dokumen54 halamanWound Assessment: Pusat Perawatan Luka "Patria Care" Stikes Patria Husada BLITAR 2019pristanti tantiBelum ada peringkat
- Principles of Wound Care: Professor Claire HaleDokumen20 halamanPrinciples of Wound Care: Professor Claire HaleMACPANAMERABelum ada peringkat
- Ns 313 Surgical Nursing: Wound Dressing TechniquesDokumen48 halamanNs 313 Surgical Nursing: Wound Dressing TechniquesZabron LuhendeBelum ada peringkat
- Chapter-2 Skin IntegrityDokumen91 halamanChapter-2 Skin IntegrityDianaBelum ada peringkat
- Debridement of Pressure UlcersDokumen10 halamanDebridement of Pressure UlcersMa. Mechile MartinezBelum ada peringkat
- Clinical Procedures for Safer Patient Wound CareDokumen50 halamanClinical Procedures for Safer Patient Wound CareJan Oliver Yares100% (2)
- DR Mohit Gulati (PT)Dokumen62 halamanDR Mohit Gulati (PT)Shubha DiwakarBelum ada peringkat
- DNA RNA VirusesDokumen88 halamanDNA RNA VirusesHerlina NababanBelum ada peringkat
- 01 Nursing As A ProfessionDokumen14 halaman01 Nursing As A ProfessionHerlinaNababanBelum ada peringkat
- Autonomic Nervous System Drugs: Joy N. Bautista, RN, MPH, DRDM, MANDokumen14 halamanAutonomic Nervous System Drugs: Joy N. Bautista, RN, MPH, DRDM, MANHerlina NababanBelum ada peringkat
- Sedative-Hypnotics: Joy N Bautista, RN, MPH, DRDMDokumen8 halamanSedative-Hypnotics: Joy N Bautista, RN, MPH, DRDMHerlina NababanBelum ada peringkat
- Pharma 05Dokumen7 halamanPharma 05Herlina NababanBelum ada peringkat
- Skeletal SystemDokumen125 halamanSkeletal SystemJem Pantig100% (4)
- Pharma 09Dokumen7 halamanPharma 09Herlina NababanBelum ada peringkat
- MGMT Surg WoundsDokumen5 halamanMGMT Surg WoundsHerlinaNababanBelum ada peringkat
- Skin Integrity N Wound CareDokumen26 halamanSkin Integrity N Wound CareHerlina NababanBelum ada peringkat
- Diabetes Mellitus HomeopathyDokumen52 halamanDiabetes Mellitus HomeopathykshahulhameedBelum ada peringkat
- Asam Traneksamat Untuk KulitDokumen2 halamanAsam Traneksamat Untuk KulitmonitamiftahBelum ada peringkat
- Edited Psyche DrugsDokumen49 halamanEdited Psyche Drugsa_lavina02Belum ada peringkat
- Topic 1 PseudomonashhjjunDokumen8 halamanTopic 1 PseudomonashhjjunRachel Marie M. GaniaBelum ada peringkat
- Willard 2007 GastroenterologíaDokumen65 halamanWillard 2007 GastroenterologíaHazel.Belum ada peringkat
- Qsar by Hansch Analysis: Faculty of Pharmaceutical Sciences, Maharshi Dayanand University, RohtakDokumen5 halamanQsar by Hansch Analysis: Faculty of Pharmaceutical Sciences, Maharshi Dayanand University, RohtakastrimentariBelum ada peringkat
- Cluster 5: Written Assignment: Before Completing and Submitting This Assignment, Have You: What You Have To DoDokumen10 halamanCluster 5: Written Assignment: Before Completing and Submitting This Assignment, Have You: What You Have To Dorishabhk28995100% (1)
- 2018 TransCode Mock Test 6-Questions PDFDokumen37 halaman2018 TransCode Mock Test 6-Questions PDFJasliya Ismail100% (7)
- Form 5 Chemistry Folio - MedicineDokumen37 halamanForm 5 Chemistry Folio - MedicineHeon50% (2)
- An Introduction To Basic Medical English Terminology 1Dokumen346 halamanAn Introduction To Basic Medical English Terminology 1bbbanyi100% (2)
- MSRT 0003Dokumen3 halamanMSRT 0003api-336525339Belum ada peringkat
- Sickle Cell: Kelompok 1 1. Alestya Febrimaharani 2. Iftah Shorayya 3. Lastri Sulastri 4. Siti ShopiaturohmahDokumen15 halamanSickle Cell: Kelompok 1 1. Alestya Febrimaharani 2. Iftah Shorayya 3. Lastri Sulastri 4. Siti ShopiaturohmahErnesta Saulina DewiBelum ada peringkat
- Introduction to Neuro MR Imaging SequencesDokumen49 halamanIntroduction to Neuro MR Imaging SequencesJess RiveraBelum ada peringkat
- TF-CBT Toolkit With Color Laminates 1.30.12Dokumen134 halamanTF-CBT Toolkit With Color Laminates 1.30.12kurniawati budi rahayu100% (5)
- NCM 100 SKILLS Nursing Process HandoutsDokumen10 halamanNCM 100 SKILLS Nursing Process HandoutsPearl IbisateBelum ada peringkat
- Hybrid Compounds As Direct Multitarget Ligands: A ReviewDokumen36 halamanHybrid Compounds As Direct Multitarget Ligands: A ReviewJames TerryBelum ada peringkat
- Spek Ven Avea Full ClioDokumen3 halamanSpek Ven Avea Full ClioRinawatiBelum ada peringkat
- Doctor's Orders and Patient Care in ICUDokumen4 halamanDoctor's Orders and Patient Care in ICUJuan Miguel OliverosBelum ada peringkat
- Dialysis Treatment Options for Kidney FailureDokumen53 halamanDialysis Treatment Options for Kidney FailureAnand P KiranBelum ada peringkat
- Answer To Ophthaproblem 2. Filamentary KeratitisDokumen1 halamanAnswer To Ophthaproblem 2. Filamentary KeratitisKoas Saraf Angkatan 96Belum ada peringkat
- Chemotherapy DrugsDokumen43 halamanChemotherapy Drugsbrigette_lagat100% (2)
- Pricelis HargaDokumen30 halamanPricelis Hargadwi mulyaningsihBelum ada peringkat
- Breast cancer visibility comparison of tomosynthesis vs digital mammographyDokumen9 halamanBreast cancer visibility comparison of tomosynthesis vs digital mammographyjackridenBelum ada peringkat
- Sudden Cardiac Death Causes and PreventionDokumen3 halamanSudden Cardiac Death Causes and PreventionGelo JosonBelum ada peringkat
- Pharmacy Critical CareDokumen136 halamanPharmacy Critical CareTohShengPoo100% (1)
- Oral Habits Retained Deciduous Teeth and Supernumeraries Premature LossDokumen4 halamanOral Habits Retained Deciduous Teeth and Supernumeraries Premature LossGem Hanna Callano ParaguaBelum ada peringkat
- Vitamin D - MedlinePlus Medical EncyclopediaDokumen4 halamanVitamin D - MedlinePlus Medical Encyclopediarameshbabu1984100% (1)
- Bosniak ClassificationDokumen19 halamanBosniak ClassificationGirish Kumar100% (1)
- Annual Report 2011 HIV NATDokumen92 halamanAnnual Report 2011 HIV NATIs-ma PontiBelum ada peringkat
- Etiology of Epilepsy PDFDokumen2 halamanEtiology of Epilepsy PDFKellieBelum ada peringkat