Anda mungkin juga menyukai
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- Reading Train 3 Student Book PDFDokumen106 halamanReading Train 3 Student Book PDFLava100% (1)
- +2014 (6.0) Guide To Pathfinder Society Organized Play DONEDokumen51 halaman+2014 (6.0) Guide To Pathfinder Society Organized Play DONEBrogan99100% (2)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- GTA Vice City WalkDokumen463 halamanGTA Vice City WalkFrank Du ToitBelum ada peringkat
- Pump Head CalculationDokumen14 halamanPump Head CalculationSolymanElsayedSolymanBelum ada peringkat
- Examination of AbdomenDokumen41 halamanExamination of AbdomenMohammad_Islam87Belum ada peringkat
- Double Wishbone Suspension System (10bme1065)Dokumen16 halamanDouble Wishbone Suspension System (10bme1065)Nikhil Gupta100% (3)
- Stomach - GastritisDokumen22 halamanStomach - GastritisaimanBelum ada peringkat
- Presentation On Sports Writing 2013-14Dokumen50 halamanPresentation On Sports Writing 2013-14henryBelum ada peringkat
- Lecture 20 CarcinogenesisDokumen84 halamanLecture 20 CarcinogenesisMohammad_Islam87100% (1)
- Floor Mounted Jib CraneDokumen2 halamanFloor Mounted Jib CraneVishnu SathyaBelum ada peringkat
- Morphopathology SET 16 Pathologies of The Gastrointestinal TractDokumen29 halamanMorphopathology SET 16 Pathologies of The Gastrointestinal TractMohammad_Islam87Belum ada peringkat
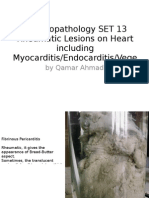
- Morphopathology SET 13 Rheumatic Lesions On Heart Including Myocarditis/Endocarditis/VegeDokumen25 halamanMorphopathology SET 13 Rheumatic Lesions On Heart Including Myocarditis/Endocarditis/VegeMohammad_Islam87Belum ada peringkat
- AnaemiaDokumen83 halamanAnaemiaMohammad_Islam87100% (2)
- Liver Curs 2009Dokumen215 halamanLiver Curs 2009Mohammad_Islam87Belum ada peringkat
- Morphopathology SET 15 Renal Pathologies: by Qamar AhmadDokumen25 halamanMorphopathology SET 15 Renal Pathologies: by Qamar AhmadMohammad_Islam87Belum ada peringkat
- Morphopathology SET 12 Cardiomyopathy (Ischemic) : by Qamar AhmadDokumen19 halamanMorphopathology SET 12 Cardiomyopathy (Ischemic) : by Qamar AhmadMohammad_Islam87Belum ada peringkat
- Morphopathology Macroscopy (Romanian-Batch)Dokumen187 halamanMorphopathology Macroscopy (Romanian-Batch)Mohammad_Islam87100% (1)
- Morphopathology SET14 Respiratory Pathologies: by Qamar AhmadDokumen18 halamanMorphopathology SET14 Respiratory Pathologies: by Qamar AhmadMohammad_Islam87Belum ada peringkat
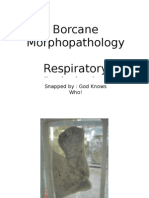
- Borcane Morphopathology Respiratory Pathologies: Snapped By: God Knows Who! Compiled By: QamarDokumen11 halamanBorcane Morphopathology Respiratory Pathologies: Snapped By: God Knows Who! Compiled By: QamarMohammad_Islam87Belum ada peringkat
- ?#ry%oefr: - J4 @,8/ MryDokumen15 halaman?#ry%oefr: - J4 @,8/ MryMohammad_Islam87Belum ada peringkat
- Macroscopy Set 10 Circulatory Disturbances: by Qamar AhmadDokumen55 halamanMacroscopy Set 10 Circulatory Disturbances: by Qamar AhmadMohammad_Islam87Belum ada peringkat
- Borcane Morphopathology Liver Pathologies: Snapped By: God Knows Who! Compiled By: QamarDokumen7 halamanBorcane Morphopathology Liver Pathologies: Snapped By: God Knows Who! Compiled By: QamarMohammad_Islam87100% (1)
- Workshop 19Dokumen3 halamanWorkshop 19Mohammad_Islam87Belum ada peringkat
- Conditions Presenting With Abdominal PainDokumen69 halamanConditions Presenting With Abdominal PainaimanBelum ada peringkat
- Borcane Morphopathology Various Pathologies: Snapped By: God Knows Who! Compiled By: QamarDokumen7 halamanBorcane Morphopathology Various Pathologies: Snapped By: God Knows Who! Compiled By: QamarMohammad_Islam87Belum ada peringkat
- Workshop 20Dokumen2 halamanWorkshop 20Mohammad_Islam87Belum ada peringkat
- Morphopatholgy Set 9 Circulatory Disturbances: by Qamar AhmadDokumen24 halamanMorphopatholgy Set 9 Circulatory Disturbances: by Qamar AhmadMohammad_Islam87Belum ada peringkat
- Physical Signs of The AbdomenDokumen93 halamanPhysical Signs of The AbdomenaimanBelum ada peringkat
- Workshop 18Dokumen4 halamanWorkshop 18Mohammad_Islam87Belum ada peringkat
- Morphopathology Set 11 Atherosclerosis and Other Cardiaovascular DisordersDokumen21 halamanMorphopathology Set 11 Atherosclerosis and Other Cardiaovascular DisordersMohammad_Islam87Belum ada peringkat
- Morphopathology Set 8 Melanocytic Tumors: by Qamar AhmadDokumen54 halamanMorphopathology Set 8 Melanocytic Tumors: by Qamar AhmadMohammad_Islam87Belum ada peringkat
- STOMACCURS2Dokumen12 halamanSTOMACCURS2Mohammad_Islam87Belum ada peringkat
- Workshop 17Dokumen4 halamanWorkshop 17Mohammad_Islam87Belum ada peringkat
- Peptic Ulcer DiseaseDokumen54 halamanPeptic Ulcer DiseaseMohammad_Islam87Belum ada peringkat
- 8950P230 Sample PDFDokumen6 halaman8950P230 Sample PDFKimberly Binay-anBelum ada peringkat
- Chess TacticsDokumen172 halamanChess Tacticsأبو الطيب المتنبي100% (1)
- Tattoo Final ListDokumen15 halamanTattoo Final ListRikardo JumawanBelum ada peringkat
- Workout 1 (Monday) : Chest, Shoulders, TricepsDokumen7 halamanWorkout 1 (Monday) : Chest, Shoulders, Tricepsdogra.diwakar8365Belum ada peringkat
- Est N1522CDokumen1 halamanEst N1522CPrastyo TyoBelum ada peringkat
- FormulasDokumen20 halamanFormulasRishit MevadaBelum ada peringkat
- Jeff Tamolang Ballistic1Dokumen6 halamanJeff Tamolang Ballistic1edionBelum ada peringkat
- Manual Muscle Testing of Shoulder RegionDokumen8 halamanManual Muscle Testing of Shoulder RegionSyeda Bint E KhalilBelum ada peringkat
- Name:Khok Chiu Yin Kelas: HSK 1 DVM Speech Outline: Speech Title /topic Opening Attention GetterDokumen3 halamanName:Khok Chiu Yin Kelas: HSK 1 DVM Speech Outline: Speech Title /topic Opening Attention GetterflakkaBelum ada peringkat
- History of LexuxDokumen23 halamanHistory of LexuxRajanikantJadhavBelum ada peringkat
- B. Movement B. Personal C. ReferenceDokumen4 halamanB. Movement B. Personal C. ReferenceKhánh Linh LêBelum ada peringkat
- Lamborghini Gallardo Superlegerra LP-570 PapercraftDokumen3 halamanLamborghini Gallardo Superlegerra LP-570 PapercraftFelixz Giatama100% (1)
- Test 9th GradeDokumen3 halamanTest 9th Gradepocoyo potacioBelum ada peringkat
- Steyn City BrochureDokumen36 halamanSteyn City BrochureCorey AcevedoBelum ada peringkat
- Jotun's TombDokumen2 halamanJotun's TombLloyd CollinsBelum ada peringkat
- Today Our Learning TopicDokumen13 halamanToday Our Learning Topictrisha_130Belum ada peringkat
- DLP2 Pe6Dokumen2 halamanDLP2 Pe6Jesson AlbaranBelum ada peringkat
- Exercise of Body MechanicsDokumen4 halamanExercise of Body Mechanicslostloved7Belum ada peringkat
- 2010 LeftySpeed Oms en 0Dokumen29 halaman2010 LeftySpeed Oms en 0Discord ShadowBelum ada peringkat
- Check With Track For Official Betting Numbers and Post PositionsDokumen11 halamanCheck With Track For Official Betting Numbers and Post PositionsAsbury Park PressBelum ada peringkat
- Frequency Tables and Dot PlotsDokumen6 halamanFrequency Tables and Dot PlotsdnyBelum ada peringkat
- Fest Ticket Monster Hunter World WikiDokumen1 halamanFest Ticket Monster Hunter World WikiferdynandcBelum ada peringkat
- Last Update: 07.05.20 Source of Data: Eurostat: Producer Prices in Industry, Total - Annual Data (Sts - Inpp - A)Dokumen2 halamanLast Update: 07.05.20 Source of Data: Eurostat: Producer Prices in Industry, Total - Annual Data (Sts - Inpp - A)ralucaBelum ada peringkat