Anda mungkin juga menyukai
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (890)
- Cardiac MurmursDokumen53 halamanCardiac MurmursdrgashokBelum ada peringkat
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Heart Sounds and MurmursDokumen38 halamanHeart Sounds and MurmursLaura Moise100% (5)
- 12 Lead STEMI MimicsDokumen22 halaman12 Lead STEMI MimicscornondaBelum ada peringkat
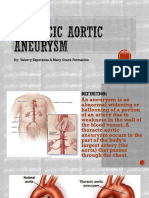
- Thoracic Aortic AneurysmDokumen17 halamanThoracic Aortic AneurysmGlyssa CabarrubiasBelum ada peringkat
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- Heart BlockDokumen26 halamanHeart BlockMihir Patel86% (7)
- ECGInterpretation Cheat SheetDokumen1 halamanECGInterpretation Cheat SheetTom Mallinson100% (1)
- 用-PSYCHOTHERAPYDokumen103 halaman用-PSYCHOTHERAPYsanjivdas100% (3)
- External HerniaDokumen136 halamanExternal Herniasanjivdas100% (1)
- Rheumatic Fever and Rheumatic Heart DiseaseDokumen54 halamanRheumatic Fever and Rheumatic Heart DiseaseFian AldyBelum ada peringkat
- Bias and ConfoundingDokumen27 halamanBias and ConfoundingsanjivdasBelum ada peringkat
- Bias and ConfoundingDokumen27 halamanBias and ConfoundingsanjivdasBelum ada peringkat
- Cardiac Rehabilitation ProtocolDokumen5 halamanCardiac Rehabilitation Protocolmarkhabm100% (1)
- Glomerular DiseaseDokumen61 halamanGlomerular DiseasesanjivdasBelum ada peringkat
- Referat Hipertensi - GeriatriDokumen21 halamanReferat Hipertensi - GeriatriAndrew SoerijadiBelum ada peringkat
- 9 The Post Anesthesia Care UnitDokumen77 halaman9 The Post Anesthesia Care Unitsanjivdas100% (1)
- Gestational Trophoblastic DiseaseDokumen71 halamanGestational Trophoblastic Diseasesanjivdas0% (1)
- 3 NeuroDokumen16 halaman3 NeurosanjivdasBelum ada peringkat
- 2 Lesson 2 - Iron Deficiency AnemiaDokumen25 halaman2 Lesson 2 - Iron Deficiency AnemiasanjivdasBelum ada peringkat
- 3 Lesson 3 - Aplastic AnemiaDokumen30 halaman3 Lesson 3 - Aplastic Anemiasanjivdas100% (1)
- 5lesson 5 - LeukemiaDokumen83 halaman5lesson 5 - LeukemiasanjivdasBelum ada peringkat
- 2 OrbitDokumen30 halaman2 OrbitsanjivdasBelum ada peringkat
- General Aspects of Hematopoetic SystemDokumen34 halamanGeneral Aspects of Hematopoetic SystemsanjivdasBelum ada peringkat
- Female Genital TumorDokumen55 halamanFemale Genital TumorsanjivdasBelum ada peringkat
- Acute Suppurative PeritonitisDokumen47 halamanAcute Suppurative PeritonitissanjivdasBelum ada peringkat
- Leiomyoma of The UterusDokumen17 halamanLeiomyoma of The UterussanjivdasBelum ada peringkat
- Managing & Integrating Volunteers Case Study Cyclone LarryDokumen18 halamanManaging & Integrating Volunteers Case Study Cyclone LarrysanjivdasBelum ada peringkat
- 体格检查Dokumen12 halaman体格检查sanjivdasBelum ada peringkat
- Disorder Relate of StressDokumen27 halamanDisorder Relate of StresssanjivdasBelum ada peringkat
- The Ovaries and OviductsDokumen20 halamanThe Ovaries and OviductssanjivdasBelum ada peringkat
- Chapter 1 Signs and Symptoms of Mental DisordersDokumen120 halamanChapter 1 Signs and Symptoms of Mental DisorderssanjivdasBelum ada peringkat
- En Dome Trial CarcinomaDokumen22 halamanEn Dome Trial CarcinomasanjivdasBelum ada peringkat
- Epidemiology ApplicationsDokumen39 halamanEpidemiology ApplicationssanjivdasBelum ada peringkat
- Acute Renal FailureDokumen48 halamanAcute Renal FailuresanjivdasBelum ada peringkat
- Cancer EpidemiologyDokumen22 halamanCancer EpidemiologysanjivdasBelum ada peringkat
- 1.ocular TraumaDokumen48 halaman1.ocular TraumasanjivdasBelum ada peringkat
- Chronic Renal FailureDokumen54 halamanChronic Renal Failuresanjivdas100% (3)
- Chapter 11 Aetiology of PsychiatryDokumen48 halamanChapter 11 Aetiology of PsychiatrysanjivdasBelum ada peringkat
- Urinarytract InfectionDokumen61 halamanUrinarytract InfectionsanjivdasBelum ada peringkat
- 28-Randomised Controlled Trial-YangBF 09.5.12Dokumen14 halaman28-Randomised Controlled Trial-YangBF 09.5.12sanjivdasBelum ada peringkat
- 1 SMDokumen15 halaman1 SMemmanuellagrace06Belum ada peringkat
- 2021 ESC Guidelines For The Diagnosis and Treatment of Acute and Chronic Heart FailureDokumen128 halaman2021 ESC Guidelines For The Diagnosis and Treatment of Acute and Chronic Heart Failureidirectored5438Belum ada peringkat
- New Right Bundle Branch Block As A CriterionDokumen3 halamanNew Right Bundle Branch Block As A CriterionNITACORDEIROBelum ada peringkat
- Step 2 CK NotesDokumen76 halamanStep 2 CK Noteskeyurb100% (1)
- Laporan TGL 16-07-21Dokumen46 halamanLaporan TGL 16-07-21Nenden Sri Mayang IIBelum ada peringkat
- Certified Ecg Tchnician Syllabus 2021Dokumen5 halamanCertified Ecg Tchnician Syllabus 2021Whiteboard DiscoveryBelum ada peringkat
- Bifascicular Block OverviewDokumen4 halamanBifascicular Block Overviewahmed ibrahimBelum ada peringkat
- Permanent Junctional Reciprocating Tachycardia in Children - A Multicenter Experience 2014Dokumen26 halamanPermanent Junctional Reciprocating Tachycardia in Children - A Multicenter Experience 2014Võ Từ NhấtBelum ada peringkat
- Penyuluhan Dan Pendampingan Senam Prolanis Pada Penderita Diabetes Mellitus Di Dusun I Desa Kanuna Kecamatan Kinovaro Kabupaten SigiDokumen9 halamanPenyuluhan Dan Pendampingan Senam Prolanis Pada Penderita Diabetes Mellitus Di Dusun I Desa Kanuna Kecamatan Kinovaro Kabupaten Sigisavira medinaBelum ada peringkat
- Pulmonary Edema by DR Gireesh Kumar K PDokumen16 halamanPulmonary Edema by DR Gireesh Kumar K PAETCM Emergency medicineBelum ada peringkat
- Debra Laurent HandoutDokumen23 halamanDebra Laurent Handoutrrs111rrsBelum ada peringkat
- Classification of Congenital Heart DiseaseDokumen1 halamanClassification of Congenital Heart DiseaseClaudia SanchezBelum ada peringkat
- Seminar Electrocardiogram (ECG)Dokumen32 halamanSeminar Electrocardiogram (ECG)Jamuna PatelBelum ada peringkat
- Mitral Stenosis Mitral RegurgitationDokumen4 halamanMitral Stenosis Mitral RegurgitationQonita SyafrinaBelum ada peringkat
- Medicine Review 2018 1Dokumen470 halamanMedicine Review 2018 1Norjetalexis Maningo CabreraBelum ada peringkat
- TV 2021Dokumen17 halamanTV 2021c4fcz9dj4fBelum ada peringkat
- Pem. Cardiovaskular Dr. MulyadiDokumen195 halamanPem. Cardiovaskular Dr. MulyadiBettry Ahmad100% (1)
- Doppler Systolic Signal Void in Hypertrophic Cardiomyopathy Apical Aneurysm and Severe Obstruction Without Elevated Intraventricular VelocitiesDokumen12 halamanDoppler Systolic Signal Void in Hypertrophic Cardiomyopathy Apical Aneurysm and Severe Obstruction Without Elevated Intraventricular VelocitiesAbraham PaulBelum ada peringkat
- Nursing Care For Patient With HypertensionDokumen13 halamanNursing Care For Patient With HypertensionSachin MadhukarBelum ada peringkat
- Complication of MI (Myocardial Infarction)Dokumen2 halamanComplication of MI (Myocardial Infarction)Zahid QamarBelum ada peringkat
- Week 5Dokumen4 halamanWeek 5Ashley CastroBelum ada peringkat