Anda mungkin juga menyukai
- DYI For Natural Cure of H Pylori and Gastritis at Home?Dokumen60 halamanDYI For Natural Cure of H Pylori and Gastritis at Home?gomitadelimon100% (1)
- Eat Right For Your TypeDokumen3 halamanEat Right For Your TypeDuppala Sateesh Kumar0% (2)
- Disturbances in Ingestion: Prepared By: Jan Paul Valeros Sicat, PHRN, USRNDokumen41 halamanDisturbances in Ingestion: Prepared By: Jan Paul Valeros Sicat, PHRN, USRNAriane-Gay Cristobal Duran100% (1)
- Lower GI BleedingDokumen40 halamanLower GI BleedingMohammad Firdaus100% (2)
- Solution: Mark Pimentel, MDDokumen166 halamanSolution: Mark Pimentel, MDJoanBelum ada peringkat
- CIMSR Nursing College Lesson Plan on Peptic Ulcer DiseaseDokumen11 halamanCIMSR Nursing College Lesson Plan on Peptic Ulcer Diseasemohamad dildar100% (3)
- Acute Pancreatitis: Sudden Severe Abdominal Pain Systemic UpsetDokumen40 halamanAcute Pancreatitis: Sudden Severe Abdominal Pain Systemic UpsetcoolcaesarBelum ada peringkat
- Peptic Duodenal Ulcer History, Causes, Symptoms and TreatmentDokumen106 halamanPeptic Duodenal Ulcer History, Causes, Symptoms and TreatmentCanan YilmazBelum ada peringkat
- Lecture 20 CarcinogenesisDokumen84 halamanLecture 20 CarcinogenesisMohammad_Islam87100% (1)
- Peptic Ulcer Disease: "Something Is Eating at Me"Dokumen37 halamanPeptic Ulcer Disease: "Something Is Eating at Me"bobtaguba100% (1)
- The Effects of Stress On Your BodyDokumen12 halamanThe Effects of Stress On Your BodysatishBelum ada peringkat
- Assessing & Managing Urinary Tract DisordersDokumen5 halamanAssessing & Managing Urinary Tract DisordersAlyssa Nicole CajayonBelum ada peringkat
- By DR.: Haitham Mokhtar Mohamed Abd AllahDokumen101 halamanBy DR.: Haitham Mokhtar Mohamed Abd AllahMohamed ElkadyBelum ada peringkat
- NCP For CholecystitisDokumen9 halamanNCP For Cholecystitisjmravago220% (1)
- Key Answers and Medical Surgical Nursing 1 - FINALS ExaminatiDokumen11 halamanKey Answers and Medical Surgical Nursing 1 - FINALS ExaminatiJune Dumdumaya100% (1)
- Biliary Tract Dis Pancreatitis 2015Dokumen143 halamanBiliary Tract Dis Pancreatitis 2015eiad-mahmoudBelum ada peringkat
- ReviewDokumen5 halamanReviewKristine SingsonBelum ada peringkat
- GIT OverviewDokumen108 halamanGIT OverviewNasser SalahBelum ada peringkat
- Non Variceal Upper GI Bleeding: Causes, Risk Factors, Diagnosis and ManagementDokumen66 halamanNon Variceal Upper GI Bleeding: Causes, Risk Factors, Diagnosis and ManagementsarangpbBelum ada peringkat
- Update On The Management of PancreatitisDokumen92 halamanUpdate On The Management of Pancreatitisadamu mohammadBelum ada peringkat
- ICD 10.0: K29 Condition/Disease: Gastritis Description:: SymptomDokumen3 halamanICD 10.0: K29 Condition/Disease: Gastritis Description:: SymptomvicndubBelum ada peringkat
- Dr. S.P. Hewawasam (MD) Consultant Gastroenterologist/Senior Lecturer in PhysiologyDokumen33 halamanDr. S.P. Hewawasam (MD) Consultant Gastroenterologist/Senior Lecturer in PhysiologyAjung SatriadiBelum ada peringkat
- Acute Pancreatitis GuideDokumen100 halamanAcute Pancreatitis GuideJu Lie AnnBelum ada peringkat
- Acid Peptic Disorders The Spotlight Is On!Dokumen41 halamanAcid Peptic Disorders The Spotlight Is On!Wally HoneyBelum ada peringkat
- Liver D PDFDokumen71 halamanLiver D PDFermichoBelum ada peringkat
- Exmd 509 Mcgill Stomach 2016Dokumen36 halamanExmd 509 Mcgill Stomach 2016Sora OhBelum ada peringkat
- PepticDokumen29 halamanPepticMuhammad Irfan JamilBelum ada peringkat
- Acute PancreatitisDokumen11 halamanAcute Pancreatitispeter_soósBelum ada peringkat
- Peptis Ulcer-Bs TâmDokumen27 halamanPeptis Ulcer-Bs TâmÁnh PhạmBelum ada peringkat
- PankreatitisDokumen107 halamanPankreatitisIlmiah BagusBelum ada peringkat
- Cholelithiasis and CholecystitisDokumen28 halamanCholelithiasis and Cholecystitisandreva8Belum ada peringkat
- Gatot Sugiharto, MD, Internist Faculty of Medicine, UWKS Lecture - 2010Dokumen62 halamanGatot Sugiharto, MD, Internist Faculty of Medicine, UWKS Lecture - 2010Ardi PratamaBelum ada peringkat
- Pancreatitis: Pancreatitis Is Inflammation of The Pancreas. It Occurs When Pancreatic Enzymes (Especially Trypsin)Dokumen6 halamanPancreatitis: Pancreatitis Is Inflammation of The Pancreas. It Occurs When Pancreatic Enzymes (Especially Trypsin)tianallyBelum ada peringkat
- Lecture 1part 2Dokumen50 halamanLecture 1part 2mashe1Belum ada peringkat
- Jaundice: Presented by Dr. Pollock Prepared by Christopher Edwards Tintanalli Chapter 84, Pgs. 560-561 October 2005Dokumen46 halamanJaundice: Presented by Dr. Pollock Prepared by Christopher Edwards Tintanalli Chapter 84, Pgs. 560-561 October 2005Edwin Jose SBelum ada peringkat
- Gastritis: Department of Gastroenterology General Hospital of Ningxia Medical University Si Cen MDDokumen82 halamanGastritis: Department of Gastroenterology General Hospital of Ningxia Medical University Si Cen MDAvi Themessy100% (1)
- Peptic Ulcer Disease: Erwin Budi CahyonoDokumen29 halamanPeptic Ulcer Disease: Erwin Budi Cahyonoshavira nuzulaBelum ada peringkat
- Everything You Need to Know About Peptic Ulcer DiseaseDokumen29 halamanEverything You Need to Know About Peptic Ulcer Diseasehanizah kurniaBelum ada peringkat
- Clinical Clerk Seminar Series: Approach To Gi BleedsDokumen11 halamanClinical Clerk Seminar Series: Approach To Gi BleedsAngel_Liboon_388Belum ada peringkat
- Abd PainDokumen35 halamanAbd PainHandrian RahmanBelum ada peringkat
- Based on the information provided, the most likely causative organism is Cytomegalovirus (CMV). CMV is a common opportunistic infection in HIV/AIDS patients that can cause esophageal ulcersDokumen37 halamanBased on the information provided, the most likely causative organism is Cytomegalovirus (CMV). CMV is a common opportunistic infection in HIV/AIDS patients that can cause esophageal ulcersDanielle FosterBelum ada peringkat
- Bile, Bile Duct and Pancreatic DiseaseDokumen82 halamanBile, Bile Duct and Pancreatic Diseaseshahrul rahmanBelum ada peringkat
- Peptic Ulcer DiseaseDokumen2 halamanPeptic Ulcer DiseaseAlexander EnnesBelum ada peringkat
- Peptic Ulcer Disease (PUD) : Symptomatology (Common)Dokumen12 halamanPeptic Ulcer Disease (PUD) : Symptomatology (Common)Asni LongaBelum ada peringkat
- Topics in Gastroenterology - 2014Dokumen79 halamanTopics in Gastroenterology - 2014BwatBelum ada peringkat
- "Belajar Mandiri 2.4.2" Penyakit Inslamasi Pada Saluran CernaDokumen73 halaman"Belajar Mandiri 2.4.2" Penyakit Inslamasi Pada Saluran CernaNununBelum ada peringkat
- Peptic Ulcer DiseaseDokumen98 halamanPeptic Ulcer DiseaseOmar MohammedBelum ada peringkat
- Eric Ji-Yuan Mao, MD Samir A. Shah, MD, Facg, Fasge, AgafDokumen18 halamanEric Ji-Yuan Mao, MD Samir A. Shah, MD, Facg, Fasge, AgafMuhammad GassanBelum ada peringkat
- Curs 2-3 2023Dokumen115 halamanCurs 2-3 2023Andreea GuraliucBelum ada peringkat
- Acute Pancreatitis Guide: Causes, Symptoms, TreatmentDokumen100 halamanAcute Pancreatitis Guide: Causes, Symptoms, TreatmentabelBelum ada peringkat
- Peptic Ulcer DiseaseDokumen119 halamanPeptic Ulcer DiseaseJoy LacunaBelum ada peringkat
- Peptic Ulcer DiseaseDokumen45 halamanPeptic Ulcer DiseaseChinna ChadayanBelum ada peringkat
- GI BleedDokumen28 halamanGI BleedAnn Lan100% (1)
- Pancreas and GITDokumen21 halamanPancreas and GITAbuzarBelum ada peringkat
- GIN L9 Shabot 0708Dokumen53 halamanGIN L9 Shabot 0708api-3799874Belum ada peringkat
- 4-Hepatobiliary DiseaseDokumen22 halaman4-Hepatobiliary Diseaseabdalmajeed alshammaryBelum ada peringkat
- Gastrointestinal Emergencies in Children: Magdalena Trzepizur, MDDokumen64 halamanGastrointestinal Emergencies in Children: Magdalena Trzepizur, MDlindaBelum ada peringkat
- GI Stomach PDFDokumen65 halamanGI Stomach PDFBatool SherbiniBelum ada peringkat
- Definition and Etiology: PancreatitisDokumen24 halamanDefinition and Etiology: PancreatitisAliyah Tofani PawelloiBelum ada peringkat
- Gastro 2006Dokumen66 halamanGastro 2006Nyoman TapayanaBelum ada peringkat
- Acute PancreatitisDokumen64 halamanAcute PancreatitisOleksandr RotarBelum ada peringkat
- Fever and Abdominal Pain - Causes and DiagnosisDokumen7 halamanFever and Abdominal Pain - Causes and DiagnosisgianneBelum ada peringkat
- Approach To JaundiceDokumen36 halamanApproach To JaundiceNandita ChatterjeeBelum ada peringkat
- Lect - Peptic Ulcer - 211020 - 182113Dokumen38 halamanLect - Peptic Ulcer - 211020 - 182113Puranjay ChandelBelum ada peringkat
- Peptic Ulcer of Stomach and DuodenumDokumen59 halamanPeptic Ulcer of Stomach and Duodenumchai rinBelum ada peringkat
- 2 Approach To Elevated LFTDokumen59 halaman2 Approach To Elevated LFTparik2321Belum ada peringkat
- CHOLECYSTITISDokumen6 halamanCHOLECYSTITISAnar ChuluunBelum ada peringkat
- Current and Future Developments in Surgery: Volume 2: Oesophago-gastric SurgeryDari EverandCurrent and Future Developments in Surgery: Volume 2: Oesophago-gastric SurgeryBelum ada peringkat
- Lecture 18 Upper Digestive DiseasesDokumen63 halamanLecture 18 Upper Digestive DiseasesMohammad_Islam87Belum ada peringkat
- Lecture 17 DiabetesDokumen51 halamanLecture 17 DiabetesMohammad_Islam87Belum ada peringkat
- Physiopathology SyllabusDokumen1 halamanPhysiopathology SyllabusMohammad_Islam87Belum ada peringkat
- The BreastDokumen72 halamanThe BreastMohammad_Islam87Belum ada peringkat
- Plastic SurgeryDokumen11 halamanPlastic SurgeryMohammad_Islam87Belum ada peringkat
- AnaemiaDokumen83 halamanAnaemiaMohammad_Islam87100% (2)
- Abdominal HerniaeDokumen66 halamanAbdominal HerniaeMohammad_Islam87Belum ada peringkat
- Pharmacology Lecture 19-5-2009, NSAIDSDokumen19 halamanPharmacology Lecture 19-5-2009, NSAIDSMohammad_Islam87Belum ada peringkat
- The LymphomasDokumen46 halamanThe LymphomasMohammad_Islam87Belum ada peringkat
- Liver Curs 2009Dokumen215 halamanLiver Curs 2009Mohammad_Islam87Belum ada peringkat
- Curst Um Abd EnglDokumen10 halamanCurst Um Abd EnglMohammad_Islam87Belum ada peringkat
- Pharmacology Lecture 12-5-2009, OpiodsDokumen18 halamanPharmacology Lecture 12-5-2009, OpiodsMohammad_Islam87Belum ada peringkat
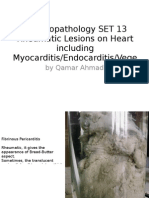
- Morphopathology SET 13 Rheumatic Lesions On Heart Including Myocarditis/Endocarditis/VegeDokumen25 halamanMorphopathology SET 13 Rheumatic Lesions On Heart Including Myocarditis/Endocarditis/VegeMohammad_Islam87Belum ada peringkat
- Morphopathology SET 15 Renal Pathologies: by Qamar AhmadDokumen25 halamanMorphopathology SET 15 Renal Pathologies: by Qamar AhmadMohammad_Islam87Belum ada peringkat
- Morphopathology SET14 Respiratory Pathologies: by Qamar AhmadDokumen18 halamanMorphopathology SET14 Respiratory Pathologies: by Qamar AhmadMohammad_Islam87Belum ada peringkat
- Pharmacology Lecture 5-5-2009Dokumen15 halamanPharmacology Lecture 5-5-2009Mohammad_Islam87Belum ada peringkat
- Morphopathology SET 16 Pathologies of The Gastrointestinal TractDokumen29 halamanMorphopathology SET 16 Pathologies of The Gastrointestinal TractMohammad_Islam87Belum ada peringkat
- Borcane TumorDokumen14 halamanBorcane TumorMohammad_Islam87Belum ada peringkat
- Morphopathology Macroscopy (Romanian-Batch)Dokumen187 halamanMorphopathology Macroscopy (Romanian-Batch)Mohammad_Islam87100% (1)
- Morphopathology SET 12 Cardiomyopathy (Ischemic) : by Qamar AhmadDokumen19 halamanMorphopathology SET 12 Cardiomyopathy (Ischemic) : by Qamar AhmadMohammad_Islam87Belum ada peringkat
- ?#ry%oefr: - J4 @,8/ MryDokumen15 halaman?#ry%oefr: - J4 @,8/ MryMohammad_Islam87Belum ada peringkat
- Workshop 20Dokumen2 halamanWorkshop 20Mohammad_Islam87Belum ada peringkat
- Borcane Morphopathology Various Pathologies: Snapped By: God Knows Who! Compiled By: QamarDokumen7 halamanBorcane Morphopathology Various Pathologies: Snapped By: God Knows Who! Compiled By: QamarMohammad_Islam87Belum ada peringkat
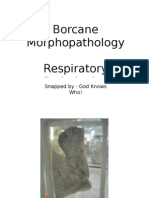
- Borcane Morphopathology Respiratory Pathologies: Snapped By: God Knows Who! Compiled By: QamarDokumen11 halamanBorcane Morphopathology Respiratory Pathologies: Snapped By: God Knows Who! Compiled By: QamarMohammad_Islam87Belum ada peringkat
- Pharmacology Lecture Diuretic Agents (High Quality)Dokumen15 halamanPharmacology Lecture Diuretic Agents (High Quality)Mohammad_Islam87Belum ada peringkat
- Borcane Morphopathology Liver Pathologies: Snapped By: God Knows Who! Compiled By: QamarDokumen7 halamanBorcane Morphopathology Liver Pathologies: Snapped By: God Knows Who! Compiled By: QamarMohammad_Islam87100% (1)
- Workshop 19Dokumen3 halamanWorkshop 19Mohammad_Islam87Belum ada peringkat
- Conditions Presenting With Abdominal PainDokumen69 halamanConditions Presenting With Abdominal PainaimanBelum ada peringkat
- Engl BUN - EditDokumen167 halamanEngl BUN - EditMohammad_Islam87Belum ada peringkat
- Surgery 2 Exam ReviewDokumen3 halamanSurgery 2 Exam ReviewValerie Gonzaga-CarandangBelum ada peringkat
- من جامعة الأردن PDFDokumen266 halamanمن جامعة الأردن PDFyousefBelum ada peringkat
- LansoprazoleDokumen3 halamanLansoprazoleTrisna meyanaBelum ada peringkat
- A New PPI, Ilaprazole (Tablet) Compared With Omeprazole in The Treatment of Duodenal UlcerDokumen8 halamanA New PPI, Ilaprazole (Tablet) Compared With Omeprazole in The Treatment of Duodenal UlcerRetno DanarwatiBelum ada peringkat
- Non-Steroidal Anti-Inflammatory Drugs (NSAID) : The Risks and BenefitsDokumen7 halamanNon-Steroidal Anti-Inflammatory Drugs (NSAID) : The Risks and Benefitsdhiraj.2367Belum ada peringkat
- Mallory-Weiss Syndrome Causes Bleeding from Esophageal TearsDokumen26 halamanMallory-Weiss Syndrome Causes Bleeding from Esophageal TearsNi MoBelum ada peringkat
- Gatehouse Report PDFDokumen978 halamanGatehouse Report PDFTauseek RangrejBelum ada peringkat
- 20513933Dokumen8 halaman20513933denitriBelum ada peringkat
- Selective and Total Vagotomy Plus Pyloroplasty:: Comparative Gastric Secretion in Dogs Evesht, CharmlDokumen5 halamanSelective and Total Vagotomy Plus Pyloroplasty:: Comparative Gastric Secretion in Dogs Evesht, CharmlAlexander VigenBelum ada peringkat
- Pharmacology of GITDokumen21 halamanPharmacology of GITAlnzeer6Belum ada peringkat
- Drug Study Pre OpDokumen6 halamanDrug Study Pre OpgiaBelum ada peringkat
- GastritisDokumen4 halamanGastritisMandalaa SaputraBelum ada peringkat
- Prospective, Retrospective, and Cross-Sectional Studies: Patrick BrehenyDokumen17 halamanProspective, Retrospective, and Cross-Sectional Studies: Patrick BrehenyGracie RobbieBelum ada peringkat
- Cytotec 200 Microgram Tablets MisoprostolDokumen7 halamanCytotec 200 Microgram Tablets Misoprostolpharmacia1.comBelum ada peringkat
- Ppi Guidance Apr 17 Post GWH CommentsDokumen4 halamanPpi Guidance Apr 17 Post GWH CommentsAnonymous MRcQuQODBelum ada peringkat
- Medical Terminology A Living Language 5Th Edition Fremgen Test Bank Full Chapter PDFDokumen67 halamanMedical Terminology A Living Language 5Th Edition Fremgen Test Bank Full Chapter PDFdonaldbau62h100% (9)
- Floating Microspheres ReviewDokumen11 halamanFloating Microspheres ReviewAgus Agus Syamsur RijalBelum ada peringkat
- 3rd SemesterDokumen22 halaman3rd Semesterkrishnaptvm2004Belum ada peringkat
- Major 2Dokumen7 halamanMajor 2Demmie Marie R. FerminBelum ada peringkat
- Siddhamruta Rasa in AmlapittaDokumen8 halamanSiddhamruta Rasa in AmlapittamilindBelum ada peringkat
- Comprehensive 2A Cgfns Boot CampDokumen107 halamanComprehensive 2A Cgfns Boot CampmonmonBelum ada peringkat
- Complementary Therapies in Clinical PracticeDokumen7 halamanComplementary Therapies in Clinical PracticeChetan AmberkarBelum ada peringkat