Anda mungkin juga menyukai
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Wreck It Ralph ScreenplayDokumen114 halamanWreck It Ralph ScreenplayRebekah Sommerville100% (4)
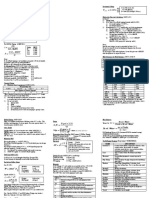
- Quick Reference CardDokumen3 halamanQuick Reference Cardaslam.ambBelum ada peringkat
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- (Tony Sato) Ariocarpus. Hand Book PDFDokumen93 halaman(Tony Sato) Ariocarpus. Hand Book PDFOsmarUrielReyesAscencioBelum ada peringkat
- ExtraDokumen3 halamanExtraaman100% (1)
- Chartering Terms ExplainedDokumen49 halamanChartering Terms Explainedbrett1856Belum ada peringkat
- REGULATIONS FOR SHIPSDokumen62 halamanREGULATIONS FOR SHIPSBasong SanBelum ada peringkat
- HUMSS - Q3 - Trends - Mod5 - Global Networks Part 1Dokumen24 halamanHUMSS - Q3 - Trends - Mod5 - Global Networks Part 1Chernie Deroma Obsenares67% (6)
- Kohler RRT ManualDokumen40 halamanKohler RRT Manualjmh488100% (1)
- Fluent-Intro 16.0 L02 IntroCFD PDFDokumen45 halamanFluent-Intro 16.0 L02 IntroCFD PDFAnonymous 8209ZTBelum ada peringkat
- Cat Marine Engine ProgramDokumen4 halamanCat Marine Engine ProgramRobert BeddingfieldBelum ada peringkat
- Energy Engineering and Management For Building SystemDokumen288 halamanEnergy Engineering and Management For Building SystemJivan BadaghaBelum ada peringkat
- Evaluation of Homocysteine Level As A RiskDokumen7 halamanEvaluation of Homocysteine Level As A RiskIsnawan WidyayantoBelum ada peringkat
- Disorders of The Spinal CordDokumen9 halamanDisorders of The Spinal CordIsnawan WidyayantoBelum ada peringkat
- LGS MedscapeDokumen14 halamanLGS MedscapeIsnawan WidyayantoBelum ada peringkat
- Assessment and Management of Acute Low Back PainDokumen12 halamanAssessment and Management of Acute Low Back PainIsnawan WidyayantoBelum ada peringkat
- Serum BDNF Levels in Post Stroke Depression-Li2014Dokumen7 halamanSerum BDNF Levels in Post Stroke Depression-Li2014Isnawan WidyayantoBelum ada peringkat
- UNAIDS Global Report 2013 enDokumen198 halamanUNAIDS Global Report 2013 enWindy MentariiBelum ada peringkat
- Stroke-2015-Guidelines For The Management of Patients With Unruptured Intracranial AneurysmsDokumen36 halamanStroke-2015-Guidelines For The Management of Patients With Unruptured Intracranial AneurysmsIsnawan WidyayantoBelum ada peringkat
- Stroke 2013 Qureshi S67 9Dokumen4 halamanStroke 2013 Qureshi S67 9Isnawan WidyayantoBelum ada peringkat
- Global HIV/AIDS Estimates 2013 SummaryDokumen11 halamanGlobal HIV/AIDS Estimates 2013 SummaryIsnawan WidyayantoBelum ada peringkat
- Serum BDNF Levels in Post Stroke Depression-Li2014Dokumen9 halamanSerum BDNF Levels in Post Stroke Depression-Li2014Isnawan WidyayantoBelum ada peringkat
- Effectiveness, TolerabilityDokumen38 halamanEffectiveness, TolerabilityIsnawan WidyayantoBelum ada peringkat
- Stroke-2015-Guidelines For The Early Management of Patient With Acute Ischemic Stroke Regarding Endovasculat TreatmentDokumen17 halamanStroke-2015-Guidelines For The Early Management of Patient With Acute Ischemic Stroke Regarding Endovasculat TreatmentIsnawan WidyayantoBelum ada peringkat
- Dietary Fiber and CardiovascularDokumen12 halamanDietary Fiber and CardiovascularIsnawan WidyayantoBelum ada peringkat
- Factor Xiii MedscapeDokumen35 halamanFactor Xiii MedscapeIsnawan WidyayantoBelum ada peringkat
- Stroke 2006 Tsivgoulis 1913 6Dokumen5 halamanStroke 2006 Tsivgoulis 1913 6Isnawan WidyayantoBelum ada peringkat
- Epilepsy Surgery in Indonesia Achieving Better Result With Limited ResourcesDokumen6 halamanEpilepsy Surgery in Indonesia Achieving Better Result With Limited ResourcesIsnawan WidyayantoBelum ada peringkat
- Dr. Retna-New Antiplatelet For Secondary Stroke PreventionDokumen40 halamanDr. Retna-New Antiplatelet For Secondary Stroke PreventionIsnawan WidyayantoBelum ada peringkat
- Dietary Fiber and Coronary Heart DiseaseDokumen7 halamanDietary Fiber and Coronary Heart DiseaseIsnawan WidyayantoBelum ada peringkat
- Tolosa Hunt MedscapeDokumen8 halamanTolosa Hunt MedscapeIsnawan WidyayantoBelum ada peringkat
- Referensi OADokumen36 halamanReferensi OAIsnawan WidyayantoBelum ada peringkat
- MikrobiologiDokumen11 halamanMikrobiologiIsnawan WidyayantoBelum ada peringkat
- HopeDokumen21 halamanHopeIsnawan WidyayantoBelum ada peringkat
- OsteoarthritisDokumen25 halamanOsteoarthritisVidyani AdiningtyasBelum ada peringkat
- Treatmentofaneurysmalsubarachnoidhemorrhage 090823220241 Phpapp02Dokumen17 halamanTreatmentofaneurysmalsubarachnoidhemorrhage 090823220241 Phpapp02Isnawan WidyayantoBelum ada peringkat
- THS JurnalDokumen7 halamanTHS JurnalIsnawan WidyayantoBelum ada peringkat
- Referensi OADokumen36 halamanReferensi OAIsnawan WidyayantoBelum ada peringkat
- Prevention of Varicella: Recommendations of The Advisory Committee On Immunization Practices (ACIP)Dokumen35 halamanPrevention of Varicella: Recommendations of The Advisory Committee On Immunization Practices (ACIP)Isnawan WidyayantoBelum ada peringkat
- American College of Rheumatology 2012 Recommendations For The Use of Nonpharmacologic and Pharmacologic Therapies in Osteoarthritis of The Hand, Hip, and KneeDokumen10 halamanAmerican College of Rheumatology 2012 Recommendations For The Use of Nonpharmacologic and Pharmacologic Therapies in Osteoarthritis of The Hand, Hip, and KneeAissyiyah Nur An NisaBelum ada peringkat
- Diabetes - NeuropathyDokumen2 halamanDiabetes - NeuropathyIsnawan WidyayantoBelum ada peringkat
- Complete Blood Count (CBC) Normal Laboratory Study Values: DefinitionDokumen6 halamanComplete Blood Count (CBC) Normal Laboratory Study Values: DefinitionGlare RhayneBelum ada peringkat
- RFP Master PlanDokumen9 halamanRFP Master PlanakhilchibberBelum ada peringkat
- Cast in Situ Pile Design by MurthyDokumen3 halamanCast in Situ Pile Design by MurthyQuazi ShammasBelum ada peringkat
- 4 Tutorial Present Worth AnalysisDokumen4 halaman4 Tutorial Present Worth AnalysisMuhamad SyazwanBelum ada peringkat
- Tzu Chi Medical Journal: Xiao-Jun Lin, I-Mei Lin, Sheng-Yu FanDokumen5 halamanTzu Chi Medical Journal: Xiao-Jun Lin, I-Mei Lin, Sheng-Yu Fanperisici4_535458722Belum ada peringkat
- Modelacion UreaDokumen20 halamanModelacion UreaJesus Enrique Alfonzo RiveroBelum ada peringkat
- q4_tleDokumen65 halamanq4_tleAngelica TaerBelum ada peringkat
- 842e In001 - en PDokumen4 halaman842e In001 - en PNilson Eduardo TorresBelum ada peringkat
- Abb 60 PVS-TLDokumen4 halamanAbb 60 PVS-TLNelson Jesus Calva HernandezBelum ada peringkat
- BRP-1 Final Report Borjan Private LimitedDokumen38 halamanBRP-1 Final Report Borjan Private LimitedArsalan IqbalBelum ada peringkat
- Installation Manual-Perfect YORKDokumen19 halamanInstallation Manual-Perfect YORKjesBelum ada peringkat
- CS410 Series and CS417: User's GuideDokumen209 halamanCS410 Series and CS417: User's Guident11Belum ada peringkat
- Donna's Score During The Third Quarter ExaminationDokumen7 halamanDonna's Score During The Third Quarter ExaminationGeraldine Valdez CacabilosBelum ada peringkat
- G9_Q4_W2_MODDokumen4 halamanG9_Q4_W2_MODKkkkkBelum ada peringkat
- Tuto Traktor Arduino enDokumen11 halamanTuto Traktor Arduino enlexetaBelum ada peringkat
- 2 13 Ionisation EnergiesDokumen6 halaman2 13 Ionisation EnergiesRobertLiu100% (2)
- BGMEA University of Fashion & Technology (BUFT)Dokumen9 halamanBGMEA University of Fashion & Technology (BUFT)RIFAT HASANBelum ada peringkat
- CBSE Class XII Mathematics - Inverse Trigonometric Functions Assignment 2 PDFDokumen4 halamanCBSE Class XII Mathematics - Inverse Trigonometric Functions Assignment 2 PDFPooja KathuriaBelum ada peringkat
- Bhs Inggris A - SoalDokumen9 halamanBhs Inggris A - SoalKhaerul AnamBelum ada peringkat