Anda mungkin juga menyukai
- Escalona Arranz2010Dokumen7 halamanEscalona Arranz2010Ivor Wiguna Hartanto WilopoBelum ada peringkat
- J Eururo 2020 09 046Dokumen20 halamanJ Eururo 2020 09 046Ivor Wiguna Hartanto WilopoBelum ada peringkat
- Nihms 7136222Dokumen43 halamanNihms 7136222Ivor Wiguna Hartanto WilopoBelum ada peringkat
- J Jamcollsurg 2016 03 043Dokumen29 halamanJ Jamcollsurg 2016 03 043Ivor Wiguna Hartanto WilopoBelum ada peringkat
- Vanreijen 2019Dokumen10 halamanVanreijen 2019Ivor Wiguna Hartanto WilopoBelum ada peringkat
- Jama 1965 03080030024005Dokumen3 halamanJama 1965 03080030024005Ivor Wiguna Hartanto WilopoBelum ada peringkat
- Criterios de Tokio 2018Dokumen14 halamanCriterios de Tokio 2018Luis CoraspeBelum ada peringkat
- Lerch 2020 AchillestendonDokumen10 halamanLerch 2020 AchillestendonIvor Wiguna Hartanto WilopoBelum ada peringkat
- Piis1078588418300807 PDFDokumen62 halamanPiis1078588418300807 PDFPrasojo JojoBelum ada peringkat
- Ournal of Linical Ncology: PurposeDokumen7 halamanOurnal of Linical Ncology: PurposeIvor Wiguna Hartanto WilopoBelum ada peringkat
- 8th Edition of The AJCC - TNM Staging System of Thyroid Cancer - What To Expect (ITCO#2)Dokumen5 halaman8th Edition of The AJCC - TNM Staging System of Thyroid Cancer - What To Expect (ITCO#2)Valentina IndahBelum ada peringkat
- HTDokumen17 halamanHTIvor Wiguna Hartanto WilopoBelum ada peringkat
- 2019 AMFEK Guideline & Application FormDokumen6 halaman2019 AMFEK Guideline & Application FormIvor Wiguna Hartanto WilopoBelum ada peringkat
- Jamafacial 2018 0411Dokumen2 halamanJamafacial 2018 0411Ivor Wiguna Hartanto WilopoBelum ada peringkat
- Nutrition PostoperativeDokumen47 halamanNutrition PostoperativeAnonymous 86gki5Belum ada peringkat
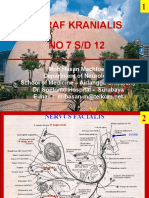
- Clerk05 Nervi KranialisDokumen14 halamanClerk05 Nervi KranialisIvor Wiguna Hartanto WilopoBelum ada peringkat
- ASN NKDEP CKD in Primary Care Presentation 2-08Dokumen33 halamanASN NKDEP CKD in Primary Care Presentation 2-08Маnal AlJobranBelum ada peringkat
- Dive MedDokumen37 halamanDive MedIvor Wiguna Hartanto WilopoBelum ada peringkat
- Hep Education 101Dokumen20 halamanHep Education 101Ivor Wiguna Hartanto WilopoBelum ada peringkat
- Petal Design 2 1Dokumen1 halamanPetal Design 2 1Ivor Wiguna Hartanto WilopoBelum ada peringkat
- FAGOSITOSISDokumen4 halamanFAGOSITOSISIvor Wiguna Hartanto WilopoBelum ada peringkat
- Craft Templates by Noella MzinzaDokumen1 halamanCraft Templates by Noella MzinzaIvor Wiguna Hartanto WilopoBelum ada peringkat
- Vetteth Chronic Kidney DiseaseDokumen35 halamanVetteth Chronic Kidney DiseaseIvor Wiguna Hartanto WilopoBelum ada peringkat
- Petal Design 3 PDFDokumen1 halamanPetal Design 3 PDFIvor Wiguna Hartanto WilopoBelum ada peringkat
- Chronic Kidney DiseaseDokumen24 halamanChronic Kidney DiseasepradeepnagdaBelum ada peringkat
- DbudibqwhDokumen2 halamanDbudibqwhIvor Wiguna Hartanto WilopoBelum ada peringkat
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5784)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (890)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (72)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Chick Lit: It's not a Gum, it's a Literary TrendDokumen2 halamanChick Lit: It's not a Gum, it's a Literary TrendspringzmeBelum ada peringkat
- Educating The PosthumanDokumen50 halamanEducating The PosthumanCatherine BrugelBelum ada peringkat
- Land-Use PlanningDokumen15 halamanLand-Use PlanningCiara MaryBelum ada peringkat
- Classification of MatterDokumen2 halamanClassification of Matterapi-280247238Belum ada peringkat
- Vivaldi - Genuis of BaroqueDokumen279 halamanVivaldi - Genuis of Baroqueilcanto100% (4)
- PrognosisDokumen7 halamanPrognosisprabadayoeBelum ada peringkat
- Solution Manual For Contemporary Project Management 4th EditionDokumen15 halamanSolution Manual For Contemporary Project Management 4th EditionDanaAllendzcfa100% (77)
- Quantitative Aptitude-More Exercise Questions Updated On Jul 2019Dokumen4 halamanQuantitative Aptitude-More Exercise Questions Updated On Jul 2019SANAMGI BHAVYABelum ada peringkat
- Chime Primary School Brochure TemplateDokumen1 halamanChime Primary School Brochure TemplateNita HanifahBelum ada peringkat
- Lorain Schools CEO Finalist Lloyd MartinDokumen14 halamanLorain Schools CEO Finalist Lloyd MartinThe Morning JournalBelum ada peringkat
- Seismic Design Guide (2010)Dokumen102 halamanSeismic Design Guide (2010)ingcarlosgonzalezBelum ada peringkat
- Gabriel Nobre de Souza - Groningen Mini-MetropolisDokumen9 halamanGabriel Nobre de Souza - Groningen Mini-MetropolisGabrielNobredeSouzaBelum ada peringkat
- ES1 Work Panel DatasheetDokumen3 halamanES1 Work Panel DatasheetGerardo Alberto Navarro LopezBelum ada peringkat
- Math 2 Unit 9 - Probability: Lesson 1: "Sample Spaces, Subsets, and Basic Probability"Dokumen87 halamanMath 2 Unit 9 - Probability: Lesson 1: "Sample Spaces, Subsets, and Basic Probability"Anonymous BUG9KZ3100% (1)
- Laser Engrave Co2 System BJ-1390Dokumen5 halamanLaser Engrave Co2 System BJ-1390Sasa TodorovicBelum ada peringkat
- Topographic Map of Blooming GroveDokumen1 halamanTopographic Map of Blooming GroveHistoricalMapsBelum ada peringkat
- Design Process at LEGODokumen5 halamanDesign Process at LEGOkapsarcBelum ada peringkat
- Eports: India's Defiance of Religious Freedom: A Briefing On Anti-Conversion' LawsDokumen16 halamanEports: India's Defiance of Religious Freedom: A Briefing On Anti-Conversion' LawsGabriela StevensBelum ada peringkat
- 2022 - J - Chir - Nastase Managementul Neoplaziilor Pancreatice PapilareDokumen8 halaman2022 - J - Chir - Nastase Managementul Neoplaziilor Pancreatice PapilarecorinaBelum ada peringkat
- IBM Credit Corp BPR ProcessDokumen8 halamanIBM Credit Corp BPR ProcessAnubhav PuriBelum ada peringkat
- Fancy YarnsDokumen7 halamanFancy Yarnsiriarn100% (1)
- A Laboratory Experiment in Crystals and Crystal Model Building ObjectivesDokumen7 halamanA Laboratory Experiment in Crystals and Crystal Model Building ObjectivesrajaaBelum ada peringkat
- ENVPEP1412003Dokumen5 halamanENVPEP1412003south adventureBelum ada peringkat
- Transistor Amplifier Operating ParametersDokumen21 halamanTransistor Amplifier Operating ParametersReddyvari VenugopalBelum ada peringkat
- User Manual - Numrolgy SoftwareDokumen14 halamanUser Manual - Numrolgy SoftwareComputershastriNoproblem0% (1)
- Tos IcuDokumen1 halamanTos IcuMary Cris RombaoaBelum ada peringkat
- All Types of Switch CommandsDokumen11 halamanAll Types of Switch CommandsKunal SahooBelum ada peringkat
- LP IV Lab Zdvzmanual Sem II fbsccAY 2019-20z 20-ConvxvzzertedDokumen96 halamanLP IV Lab Zdvzmanual Sem II fbsccAY 2019-20z 20-ConvxvzzertedVikas GuptaBelum ada peringkat
- Laboratory Manual: Semester: - ViiiDokumen15 halamanLaboratory Manual: Semester: - Viiirsingh1987Belum ada peringkat
- CH 22 Solutions ManualDokumen22 halamanCH 22 Solutions Manuallmbrn0415Belum ada peringkat