Anda mungkin juga menyukai
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (890)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- EUOGS OSCE Booklet 2020Dokumen26 halamanEUOGS OSCE Booklet 2020Amanda Leow100% (1)
- 6th Central Pay Commission Salary CalculatorDokumen15 halaman6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Congenital Glaucomas: 1. Primary 2. Iridocorneal DysgenesisDokumen12 halamanCongenital Glaucomas: 1. Primary 2. Iridocorneal DysgenesiskhadzxBelum ada peringkat
- Primary Angle-Closure Glaucoma: 1. Pathogenesis 2. ClassificationDokumen9 halamanPrimary Angle-Closure Glaucoma: 1. Pathogenesis 2. ClassificationkhadzxBelum ada peringkat
- 34 Idiopathic Spec Uveitis SyndromeDokumen8 halaman34 Idiopathic Spec Uveitis SyndromekhadzxBelum ada peringkat
- Acquired 2. Isolated Familial Ectopia Lentis 3. Associated With Systemic SyndromesDokumen8 halamanAcquired 2. Isolated Familial Ectopia Lentis 3. Associated With Systemic SyndromeskhadzxBelum ada peringkat
- 12conjunctival TumoursDokumen12 halaman12conjunctival TumourskhadzxBelum ada peringkat
- Congenital Cataract: 1. Important FactsDokumen13 halamanCongenital Cataract: 1. Important FactskhadzxBelum ada peringkat
- Abnormal Lens ShapeDokumen4 halamanAbnormal Lens ShapekhadzxBelum ada peringkat
- 09conjunctival InfectionsDokumen11 halaman09conjunctival InfectionskhadzxBelum ada peringkat
- 28primary Open Angle GlaucomaDokumen21 halaman28primary Open Angle GlaucomakhadzxBelum ada peringkat
- 13 Peripheral Corneal InflamDokumen5 halaman13 Peripheral Corneal InflamkhadzxBelum ada peringkat
- 15corneal InfectionsDokumen8 halaman15corneal InfectionskhadzxBelum ada peringkat
- 02chronic Marginal BlepharitisDokumen7 halaman02chronic Marginal BlepharitiskhadzxBelum ada peringkat
- Juvenile Rheumatoid Arthritis (Jra) (Juvenile Chronic Arthritis-Jca)Dokumen70 halamanJuvenile Rheumatoid Arthritis (Jra) (Juvenile Chronic Arthritis-Jca)khadzxBelum ada peringkat
- Dermatologic DiseasesDokumen2 halamanDermatologic DiseaseskhadzxBelum ada peringkat
- Metabolic Bone DiseaseDokumen29 halamanMetabolic Bone DiseasekhadzxBelum ada peringkat
- Introduction To Forensic Medicine DR David Chumba MBCHB, Mmed (Human Pathology), Dip. For Med (Sa)Dokumen20 halamanIntroduction To Forensic Medicine DR David Chumba MBCHB, Mmed (Human Pathology), Dip. For Med (Sa)khadzxBelum ada peringkat
- Disorders of Eye LashesDokumen8 halamanDisorders of Eye LasheskhadzxBelum ada peringkat
- Ndiang'Ui: Unexpected Deaths 24 September 2009Dokumen25 halamanNdiang'Ui: Unexpected Deaths 24 September 2009khadzxBelum ada peringkat
- Chronic Osteomyelitis in Early Infancy: Presenter: DR Maina Discussant: DR Mogire (Orthopedic Surgeon)Dokumen27 halamanChronic Osteomyelitis in Early Infancy: Presenter: DR Maina Discussant: DR Mogire (Orthopedic Surgeon)khadzxBelum ada peringkat
- External Fixation of The Lower Limb 2Dokumen13 halamanExternal Fixation of The Lower Limb 2khadzxBelum ada peringkat
- Introduction To Forensic Medicine DR David Chumba MBCHB, Mmed (Human Pathology), Dip. For Med (Sa)Dokumen20 halamanIntroduction To Forensic Medicine DR David Chumba MBCHB, Mmed (Human Pathology), Dip. For Med (Sa)khadzxBelum ada peringkat
- Fire Arm Injuries 4th Yr ForensicDokumen31 halamanFire Arm Injuries 4th Yr ForensickhadzxBelum ada peringkat
- Sudden Unexpected Death FMT 400Dokumen11 halamanSudden Unexpected Death FMT 400khadzxBelum ada peringkat
- Postmortem Changes and Postmortem Time IntervalDokumen24 halamanPostmortem Changes and Postmortem Time IntervalkhadzxBelum ada peringkat
- Narcotics N HallucinogensDokumen14 halamanNarcotics N HallucinogenskhadzxBelum ada peringkat
- Poisoning by MedicinesDokumen11 halamanPoisoning by MedicineskhadzxBelum ada peringkat
- Classification of Injuries FMTDokumen30 halamanClassification of Injuries FMTkhadzx100% (2)
- Malocclusion and Orthodontic Eldoret 2009Dokumen33 halamanMalocclusion and Orthodontic Eldoret 2009khadzxBelum ada peringkat
- Carbon Monoxide Poisoning 4th YrDokumen17 halamanCarbon Monoxide Poisoning 4th YrkhadzxBelum ada peringkat
- All India Institute of Medical Sciences Nagpur Department of Obstetrics and GynecologyDokumen19 halamanAll India Institute of Medical Sciences Nagpur Department of Obstetrics and GynecologySugan GavaskarBelum ada peringkat
- Developing Human Clinically Oriented Embryology 10th Edition Moore Test BankDokumen8 halamanDeveloping Human Clinically Oriented Embryology 10th Edition Moore Test Bankdrerindavisddsybrqsdmajp100% (16)
- GE 8 ETHICS Week2 9Dokumen54 halamanGE 8 ETHICS Week2 9Jay Ar OmbleroBelum ada peringkat
- 匀夀䰀䰀䄀䈀唀匀: 匀夀䰀䰀䄀䈀唀匀 䄀 䰀䤀吀夀 䰀䤀匀匀䔀刀Dokumen35 halaman匀夀䰀䰀䄀䈀唀匀: 匀夀䰀䰀䄀䈀唀匀 䄀 䰀䤀吀夀 䰀䤀匀匀䔀刀Zala pratiksha BhagvatsinhBelum ada peringkat
- BECKMANN QandADokumen32 halamanBECKMANN QandAJc Mae CuadrilleroBelum ada peringkat
- 10 Bahasa Indonesia Kasus Kehamilan MelahirkanDokumen164 halaman10 Bahasa Indonesia Kasus Kehamilan Melahirkancuuphy meryliantBelum ada peringkat
- Practice Bulletin: Medical Management of Ectopic PregnancyDokumen7 halamanPractice Bulletin: Medical Management of Ectopic PregnancyChangBelum ada peringkat
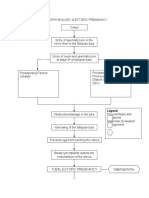
- PATHOPHYSIOLOGY of ECTOPIC PREGNANCYDokumen2 halamanPATHOPHYSIOLOGY of ECTOPIC PREGNANCYrye100% (1)
- Ats Menjawab Super Brankas Soal Unas 2020-2015Dokumen424 halamanAts Menjawab Super Brankas Soal Unas 2020-2015anton suponoBelum ada peringkat
- Question 3Dokumen19 halamanQuestion 3Anonymous LF9aizGhaBelum ada peringkat
- Spontaneous Abortion: DR - Renu SinghDokumen38 halamanSpontaneous Abortion: DR - Renu SinghRosalyn Marie SugayBelum ada peringkat
- Gynecology and Minimally Invasive TherapyDokumen2 halamanGynecology and Minimally Invasive TherapyaldyBelum ada peringkat
- Magna YeDokumen3 halamanMagna YeDiane Ronalene Cullado MagnayeBelum ada peringkat
- Rev 4 - General Gynecology 2022Dokumen28 halamanRev 4 - General Gynecology 2022Omar MohammedBelum ada peringkat
- Juli 2022Dokumen28 halamanJuli 2022Chynthea ParamithaBelum ada peringkat
- Effect of Education on Nigerian Women's Attitude Towards Family PlanningDokumen68 halamanEffect of Education on Nigerian Women's Attitude Towards Family PlanningSabanettBelum ada peringkat
- Comat NotesDokumen33 halamanComat NotesVee Mend100% (1)
- Pregnant Patient IntakeDokumen6 halamanPregnant Patient IntakeCaren MarquezBelum ada peringkat
- 6 - Cayao-Lacsam Vs Spouses RamoleteDokumen16 halaman6 - Cayao-Lacsam Vs Spouses Ramoletemartina lopezBelum ada peringkat
- Acute Appendicitis in Adults: Clinical Manifestations and DiagnosisDokumen37 halamanAcute Appendicitis in Adults: Clinical Manifestations and DiagnosisDaniela MuñozBelum ada peringkat
- CAMCAR Activity 1 - CapuchinoDokumen6 halamanCAMCAR Activity 1 - CapuchinoLawrence CapuchinoBelum ada peringkat
- Wahidin Sudirohusodo Hospital, Tuesday 19th Oct 2021 (Period October 13th - October 17th 2021)Dokumen6 halamanWahidin Sudirohusodo Hospital, Tuesday 19th Oct 2021 (Period October 13th - October 17th 2021)MirahAvishaBelum ada peringkat
- CME - Ectopic Pregnancy and Pregnancy of Unknown LocationDokumen20 halamanCME - Ectopic Pregnancy and Pregnancy of Unknown LocationQiu YipBelum ada peringkat
- OB HX MAy 6 EctopicDokumen4 halamanOB HX MAy 6 Ectopicepah1925Belum ada peringkat
- Prelim Examination MaternalDokumen23 halamanPrelim Examination MaternalAaron ConstantinoBelum ada peringkat
- Embarazo Ectopico Tubarico ACOG 2018Dokumen13 halamanEmbarazo Ectopico Tubarico ACOG 2018Jesus SuarezBelum ada peringkat
- Saudi Board OSCE2015Dokumen8 halamanSaudi Board OSCE2015Aloah122346Belum ada peringkat
- Batch Notes Gyne DDX of Vaginal BleedingDokumen3 halamanBatch Notes Gyne DDX of Vaginal BleedingPipoy AmyBelum ada peringkat
- د يزن ابو غربية نسائيةDokumen55 halamanد يزن ابو غربية نسائيةobadaBelum ada peringkat