Anda mungkin juga menyukai
- HIDUP SEHAT NABIDokumen35 halamanHIDUP SEHAT NABIHealthy7Belum ada peringkat
- DETEKSI DINI DEMAM TYPHOIDDokumen26 halamanDETEKSI DINI DEMAM TYPHOIDpradanayudaBelum ada peringkat
- SIADHDokumen11 halamanSIADHBambang UbaidiusBelum ada peringkat
- Penatalaksanaan Hipertensi Krisis COMET 2019 FinalDokumen31 halamanPenatalaksanaan Hipertensi Krisis COMET 2019 FinalLarasati Gilang Fuzi AstutiBelum ada peringkat
- Aki CKD Ferry FinalDokumen52 halamanAki CKD Ferry FinalGhina Ninditasari100% (2)
- Krisis HipertensiDokumen19 halamanKrisis HipertensiRaga ManduaruBelum ada peringkat
- Diabetes Melitus FIXDokumen44 halamanDiabetes Melitus FIXRolaRachmawaty24Belum ada peringkat
- CKD-DIABETESDokumen26 halamanCKD-DIABETESmuhdenikurniawan22Belum ada peringkat
- OPTIMIZING FOR MINI LECTURESDokumen30 halamanOPTIMIZING FOR MINI LECTURESMeilytaa Ikonic100% (1)
- DPTDokumen15 halamanDPTx22xBelum ada peringkat
- Hipertiroid Dan MolaDokumen7 halamanHipertiroid Dan MolaEdwin F. Freecss WoworBelum ada peringkat
- Soal To NefroDokumen6 halamanSoal To NefroAdinda DianBelum ada peringkat
- Referat Nefropati DiabetikDokumen21 halamanReferat Nefropati DiabetikClara Verlina100% (1)
- Diabetes Pada GeriatriDokumen25 halamanDiabetes Pada Geriatridhea100% (1)
- HIPERTENSI SEKUNDERDokumen13 halamanHIPERTENSI SEKUNDERtwulandari_14Belum ada peringkat
- SINDROM NEFROTIK PADA ANAKDokumen16 halamanSINDROM NEFROTIK PADA ANAKTrisia WindyBelum ada peringkat
- k12 & k13 - Sindroma Nefritis AkutDokumen19 halamank12 & k13 - Sindroma Nefritis AkutReaya SanyBelum ada peringkat
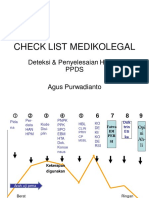
- Check List FilsafatDokumen28 halamanCheck List FilsafatrinanurbaniBelum ada peringkat
- Buku Saku Diagnosis KeperawatanDokumen6 halamanBuku Saku Diagnosis KeperawatanNURUL KOMARIAHBelum ada peringkat
- Tugas Internship RS MuhammadiyahDokumen4 halamanTugas Internship RS MuhammadiyahPutri Nisrina HamdanBelum ada peringkat
- Health Awareness - Serangan JantungDokumen19 halamanHealth Awareness - Serangan JantungMario BinsarBelum ada peringkat
- Nutrisi PGKDokumen7 halamanNutrisi PGKRaden Reyza FauziaBelum ada peringkat
- Gastroenteritis dan AnemiaDokumen49 halamanGastroenteritis dan AnemiatututBelum ada peringkat
- Kegawatdaruratan Dalam IPD Part 1Dokumen24 halamanKegawatdaruratan Dalam IPD Part 1Herizah Maulida ManurungBelum ada peringkat
- Mitral RegurgitasiDokumen19 halamanMitral RegurgitasiDyah Anugrah PratamaBelum ada peringkat
- 2.pendekatan Klinis, Diagnosis Dan Tatalaksana Nyeri SendiDokumen46 halaman2.pendekatan Klinis, Diagnosis Dan Tatalaksana Nyeri SendiEfi PujiBelum ada peringkat
- CBD AF Pada Impending Thyroid Storm IMA DR - VYADokumen27 halamanCBD AF Pada Impending Thyroid Storm IMA DR - VYAAfrilia IntanBelum ada peringkat
- Yuk Kenali HipertensiDokumen14 halamanYuk Kenali HipertensiIntan Sari WibawaBelum ada peringkat
- DETEKSI DINI DAN ALUR PENATALAKSANAANDokumen12 halamanDETEKSI DINI DAN ALUR PENATALAKSANAANgranddaeliBelum ada peringkat
- Penatalaksanaan PPOK Eksaserbasi AkutDokumen3 halamanPenatalaksanaan PPOK Eksaserbasi AkutGanistaBelum ada peringkat
- Dasar Interpretasi Foto ThoraxDokumen60 halamanDasar Interpretasi Foto ThoraxDela RohmedeskaBelum ada peringkat
- Seorang Wanita 25 Tahun G1 A0 P0 Dengan Supraventrikular Takikardi UnstableDokumen42 halamanSeorang Wanita 25 Tahun G1 A0 P0 Dengan Supraventrikular Takikardi UnstableDian KharismaBelum ada peringkat
- KDM-ABSESDokumen65 halamanKDM-ABSESagnesBelum ada peringkat
- Gangguan Elektrolit Revisi 1-1Dokumen53 halamanGangguan Elektrolit Revisi 1-1lidya agustinBelum ada peringkat
- Basic Life SupportDokumen51 halamanBasic Life SupportAnonymous YHnrc0Belum ada peringkat
- M.Haidir SOPT BBKMDokumen48 halamanM.Haidir SOPT BBKMagun100% (1)
- Contrast Induced NephropathyDokumen39 halamanContrast Induced NephropathyAjeng Sekarini100% (1)
- 11 - 207laporan Kasus Hipertrigliseridemia Berat Penderita DMDokumen3 halaman11 - 207laporan Kasus Hipertrigliseridemia Berat Penderita DMWardatun ZuhraBelum ada peringkat
- Catatan IPD Ketileng Louis ReganDokumen36 halamanCatatan IPD Ketileng Louis ReganNature InstinctBelum ada peringkat
- Chronic Heart FailureDokumen30 halamanChronic Heart FailureRian AprizaBelum ada peringkat
- Laporan Kasus 1 - Krisis HipertensDokumen32 halamanLaporan Kasus 1 - Krisis HipertensAndreas OctavianoBelum ada peringkat
- KESADARAN MENURUNDokumen22 halamanKESADARAN MENURUNKardiwonogiri KardiBelum ada peringkat
- Laporan Kasus DM Hipoglikemia Angeline GDokumen31 halamanLaporan Kasus DM Hipoglikemia Angeline GNaufal ZulfiBelum ada peringkat
- POMRDokumen6 halamanPOMREcha AhmadBelum ada peringkat
- Soal Endokrin S1Dokumen4 halamanSoal Endokrin S1nisfy mauzhaBelum ada peringkat
- Lapsus Hipertensi Emergensi AfrizalDokumen25 halamanLapsus Hipertensi Emergensi AfrizalLambert Hezekiah EddyBelum ada peringkat
- DislipidemiaDokumen19 halamanDislipidemiaAdityaGloriaMonalisaSianturiIIBelum ada peringkat
- Dasar - Dasar Kemoterapi Pada Penderita KankerDokumen42 halamanDasar - Dasar Kemoterapi Pada Penderita KankerBangkit HerlambangBelum ada peringkat
- SoptDokumen17 halamanSoptretnopuspaningtyasBelum ada peringkat
- Obat Vasopresor & Vasodilator MMDokumen23 halamanObat Vasopresor & Vasodilator MMharjunaBelum ada peringkat
- PPK PDDokumen93 halamanPPK PDGarida ZuarisaBelum ada peringkat
- Diagnosis Dan Penatalaksanaan Demam TiphoidDokumen40 halamanDiagnosis Dan Penatalaksanaan Demam TiphoidKartika RezkyBelum ada peringkat
- Kimia Kedokteran-Kesetimbangan Asam BasaDokumen30 halamanKimia Kedokteran-Kesetimbangan Asam BasaLa Ode RinaldiBelum ada peringkat
- GERDDokumen13 halamanGERDnitaBelum ada peringkat
- Asessmen Fungsi Kognitif GeriatriDokumen24 halamanAsessmen Fungsi Kognitif GeriatriAlbertus Johan Edy100% (1)
- Ginjal_SeduniaDokumen3 halamanGinjal_Seduniaanny alfianti100% (1)
- Korti SteroidDokumen8 halamanKorti SteroidAnonymous JVgpcwjgLoBelum ada peringkat
- Farmakoterapi Hipertensi - 2019Dokumen31 halamanFarmakoterapi Hipertensi - 2019aditya yulindraBelum ada peringkat
- Case Studies Discussion - HipertensiDokumen35 halamanCase Studies Discussion - HipertensievalBelum ada peringkat
- Konsensus HipertensiDokumen12 halamanKonsensus HipertensiAndromeda Pahlevi100% (2)
- SAP V Nilai-Nilai PolitikDokumen9 halamanSAP V Nilai-Nilai PolitikChanifia Izza MillataBelum ada peringkat
- Pelayanan Publik Partisipatif-1Dokumen19 halamanPelayanan Publik Partisipatif-1Chanifia Izza MillataBelum ada peringkat
- Nyeri, Clasifcation & MecanismDokumen28 halamanNyeri, Clasifcation & MecanismChanifia Izza MillataBelum ada peringkat
- Peritonitis dan AppendisitisDokumen52 halamanPeritonitis dan AppendisitisChanifia Izza MillataBelum ada peringkat
- Pelayanan Publik Ala Welfare StateDokumen19 halamanPelayanan Publik Ala Welfare StateChanifia Izza MillataBelum ada peringkat
- Konsep Dan Definisi BirokrasiDokumen6 halamanKonsep Dan Definisi BirokrasiChanifia Izza MillataBelum ada peringkat
- ADHD Merupakan Gangguan Pemusatan Perhatian Disertai HiperaktifDokumen3 halamanADHD Merupakan Gangguan Pemusatan Perhatian Disertai HiperaktifChanifia Izza MillataBelum ada peringkat
- DERMATITISDokumen15 halamanDERMATITISChanifia Izza MillataBelum ada peringkat
- Cover Referat AIDokumen5 halamanCover Referat AIChanifia Izza MillataBelum ada peringkat
- Ethics ResearchDokumen105 halamanEthics ResearchChanifia Izza MillataBelum ada peringkat
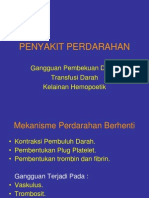
- Penyakit PerdarahanDokumen24 halamanPenyakit PerdarahanChanifia Izza MillataBelum ada peringkat
- Presus OrthoDokumen11 halamanPresus OrthoChanifia Izza MillataBelum ada peringkat
- Referat Bedah Orthopaedi JadiiDokumen32 halamanReferat Bedah Orthopaedi JadiiRezky Galuh SaputraBelum ada peringkat
- Common ColdDokumen3 halamanCommon ColdChanifia Izza MillataBelum ada peringkat
- ETIOLOGI HERNIA SCROTALISDokumen4 halamanETIOLOGI HERNIA SCROTALISN Kastim Lanyuex100% (2)
- Presus Fraktur TerbukaDokumen25 halamanPresus Fraktur TerbukaChanifia Izza MillataBelum ada peringkat
- Osteomielitis Kronik. AkbarDokumen2 halamanOsteomielitis Kronik. AkbarChanifia Izza MillataBelum ada peringkat
- MastitisDokumen5 halamanMastitisChanifia Izza MillataBelum ada peringkat
- Presus OrthoDokumen11 halamanPresus OrthoChanifia Izza MillataBelum ada peringkat
- OsteoAkutKronikDokumen20 halamanOsteoAkutKronikChanifia Izza Millata100% (1)
- PRESENTASI KASUS. Akbar N FriendsDokumen11 halamanPRESENTASI KASUS. Akbar N FriendsChanifia Izza MillataBelum ada peringkat
- Permen ESDM 01 2013Dokumen7 halamanPermen ESDM 01 2013Sumbodo SamsoniBelum ada peringkat
- Referat Rabies TBRDokumen28 halamanReferat Rabies TBRAry Nahdiyani AmaliaBelum ada peringkat
- Refrst DR JohnyDokumen87 halamanRefrst DR JohnyChanifia Izza MillataBelum ada peringkat
- SocaaaDokumen2 halamanSocaaaChanifia Izza MillataBelum ada peringkat
- Jadwal Kuliah Dan Ploting Mata Kuliah SMT Genap 2012-2013Dokumen35 halamanJadwal Kuliah Dan Ploting Mata Kuliah SMT Genap 2012-2013Chanifia Izza MillataBelum ada peringkat
- Presus RifkaDokumen10 halamanPresus RifkaChanifia Izza MillataBelum ada peringkat
- PP Presus BatuDokumen22 halamanPP Presus BatuChanifia Izza MillataBelum ada peringkat