Anda mungkin juga menyukai
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Pancreatic Cancer - Case AnalysisDokumen37 halamanPancreatic Cancer - Case AnalysisMavy CantonBelum ada peringkat
- 2015 Book Dyslipidemias PDFDokumen525 halaman2015 Book Dyslipidemias PDFvaleriaovando100% (1)
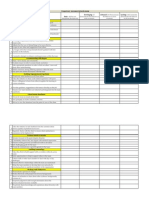
- Competency Assessment QuestionnaireDokumen2 halamanCompetency Assessment QuestionnairekurutalaBelum ada peringkat
- CBM Impact (April 2014) : Training Manager'S Name: Anil RamakrishnanDokumen2 halamanCBM Impact (April 2014) : Training Manager'S Name: Anil RamakrishnankurutalaBelum ada peringkat
- Names To Be Deleted From TracerDokumen2 halamanNames To Be Deleted From TracerkurutalaBelum ada peringkat
- Program Name Division Name Date Duration of Days TimeDokumen2 halamanProgram Name Division Name Date Duration of Days TimekurutalaBelum ada peringkat
- AnnouncementDokumen1 halamanAnnouncementkurutalaBelum ada peringkat
- SR No Division Brand: Division Wise Brands For Interview PanelDokumen1 halamanSR No Division Brand: Division Wise Brands For Interview PanelkurutalaBelum ada peringkat
- DRIVE PROGRAM (2013 - 2014) : Total Total Total TotalDokumen1 halamanDRIVE PROGRAM (2013 - 2014) : Total Total Total TotalkurutalaBelum ada peringkat
- Healtheon DetailingDokumen1 halamanHealtheon DetailingkurutalaBelum ada peringkat
- La Shield DetailingDokumen2 halamanLa Shield DetailingkurutalaBelum ada peringkat
- TOUCH Untrained Status (January 2014)Dokumen2 halamanTOUCH Untrained Status (January 2014)kurutalaBelum ada peringkat
- Ascoril Expectorant - Detailing Story InterviewsDokumen2 halamanAscoril Expectorant - Detailing Story InterviewskurutalaBelum ada peringkat
- Esoz - Detailing TalkDokumen2 halamanEsoz - Detailing TalkkurutalaBelum ada peringkat
- 08 Drug ProfileDokumen2 halaman08 Drug ProfilekurutalaBelum ada peringkat
- Yearly Calender CDG ' 12-13 FinalDokumen6 halamanYearly Calender CDG ' 12-13 FinalkurutalaBelum ada peringkat
- Glenmark CV DetailingDokumen1 halamanGlenmark CV DetailingkurutalaBelum ada peringkat
- CTV DetailingDokumen1 halamanCTV DetailingkurutalaBelum ada peringkat
- Critica VAF Detailing TalkDokumen1 halamanCritica VAF Detailing TalkkurutalaBelum ada peringkat
- Activity Report & Monthly Planner - Training Manager - AUGUST'12Dokumen4 halamanActivity Report & Monthly Planner - Training Manager - AUGUST'12kurutalaBelum ada peringkat
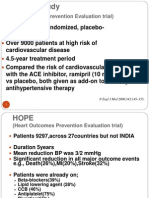
- The HOPE Study: (Heart Outcomes Prevention Evaluation Trial)Dokumen4 halamanThe HOPE Study: (Heart Outcomes Prevention Evaluation Trial)kurutalaBelum ada peringkat
- Activity Report & Monthly Planner - Training Manager - April MayDokumen4 halamanActivity Report & Monthly Planner - Training Manager - April MaykurutalaBelum ada peringkat
- Name of Employee Date of Birth (DD-MM-Yyyy) Contact NumberDokumen3 halamanName of Employee Date of Birth (DD-MM-Yyyy) Contact NumberkurutalaBelum ada peringkat
- Endocrine Physiology - Part 3 Parathyroid GlandDokumen30 halamanEndocrine Physiology - Part 3 Parathyroid GlandTerrence Beniasi CharumbiraBelum ada peringkat
- Rheumatology: With Kartik Rangaraj MDDokumen39 halamanRheumatology: With Kartik Rangaraj MDNailahRahmahBelum ada peringkat
- Rockaway Times 122916Dokumen44 halamanRockaway Times 122916Peter J. MahonBelum ada peringkat
- M010-MSI-HSE-00-PLN-02007 - Rev5 Heat Stress & Summer Working Plan PDFDokumen66 halamanM010-MSI-HSE-00-PLN-02007 - Rev5 Heat Stress & Summer Working Plan PDFEldhose VargheseBelum ada peringkat
- (NH4) 2co3Dokumen5 halaman(NH4) 2co3MuhafiBelum ada peringkat
- NURS 627 Case Study PaperDokumen11 halamanNURS 627 Case Study PaperJaclyn Strangie100% (4)
- Role of Respiratory Intermediate Care Units During The SARS-CoV-2 PandemicDokumen7 halamanRole of Respiratory Intermediate Care Units During The SARS-CoV-2 PandemicJHBelum ada peringkat
- Research Paper Thesis On Eating DisordersDokumen6 halamanResearch Paper Thesis On Eating Disordersp0zikiwyfyb2100% (1)
- BangkasDokumen5 halamanBangkasJulianne BangkasBelum ada peringkat
- Postanesthetic Aldrete Recovery Score: Original Criteria Modified Criteria Point ValueDokumen3 halamanPostanesthetic Aldrete Recovery Score: Original Criteria Modified Criteria Point ValueBonny ChristianBelum ada peringkat
- New Headway Advanced French Editable WordlistDokumen84 halamanNew Headway Advanced French Editable WordlistMaxBelum ada peringkat
- AntibioticsDokumen22 halamanAntibioticsEllen Castillo MarianoBelum ada peringkat
- Paket B Soal Listening TO US MGMP B.Inggris DKI 2023Dokumen14 halamanPaket B Soal Listening TO US MGMP B.Inggris DKI 2023X MIPA-E /10 Garnis Trie AdistyBelum ada peringkat
- Saint Francis Learning Center Foundation Inc.: For Indigenous People of ZambalesDokumen9 halamanSaint Francis Learning Center Foundation Inc.: For Indigenous People of ZambalesHector TaycoBelum ada peringkat
- Colon Cancer Preventable, Detectable With ScreeningDokumen1 halamanColon Cancer Preventable, Detectable With ScreeningAnonymous s40aYyBelum ada peringkat
- Heartjnl 2019 314702 Inline Supplementary Material 2Dokumen3 halamanHeartjnl 2019 314702 Inline Supplementary Material 2البكالوريوس المكثف فى التمريضBelum ada peringkat
- Herniated Nucleus Pulposus (HNP)Dokumen21 halamanHerniated Nucleus Pulposus (HNP)Kaye100% (1)
- Hiv Aids BookDokumen336 halamanHiv Aids BookAnshul SahuBelum ada peringkat
- Bio Toxin PathwayDokumen1 halamanBio Toxin PathwayJackie De Vries100% (1)
- Hydrogen Sulfide FactDokumen2 halamanHydrogen Sulfide FactAgriSafeBelum ada peringkat
- Lesson Plan On Pituitary Gland (Endocrine SystemDokumen37 halamanLesson Plan On Pituitary Gland (Endocrine SystemRosalyn Angcay Quintinita100% (1)
- Corona 2020: The Year of Perfect VisionDokumen5 halamanCorona 2020: The Year of Perfect VisionJorge Garcia SilesBelum ada peringkat
- For Review OAPDokumen144 halamanFor Review OAPKim John Rull NateBelum ada peringkat
- Range of Motion ExerciseDokumen8 halamanRange of Motion ExerciseAmit Martin83% (6)
- Activ One Policy WordingDokumen55 halamanActiv One Policy WordingAditya SinghBelum ada peringkat
- Food and Toxicity-Natural ToxinsDokumen47 halamanFood and Toxicity-Natural Toxinsflorina.andreea100% (1)
- Understanding The Victims of Spousal Abuse: Frank M. Ochberg, M.DDokumen6 halamanUnderstanding The Victims of Spousal Abuse: Frank M. Ochberg, M.DlovelyryBelum ada peringkat
- Nursing Selection TestDokumen3 halamanNursing Selection TestHarshita GuptaBelum ada peringkat