Anda mungkin juga menyukai
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5795)
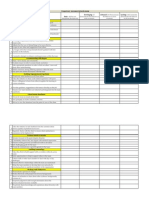
- Competency Assessment QuestionnaireDokumen2 halamanCompetency Assessment QuestionnairekurutalaBelum ada peringkat
- CBM Impact (April 2014) : Training Manager'S Name: Anil RamakrishnanDokumen2 halamanCBM Impact (April 2014) : Training Manager'S Name: Anil RamakrishnankurutalaBelum ada peringkat
- AnnouncementDokumen1 halamanAnnouncementkurutalaBelum ada peringkat
- Names To Be Deleted From TracerDokumen2 halamanNames To Be Deleted From TracerkurutalaBelum ada peringkat
- DRIVE PROGRAM (2013 - 2014) : Total Total Total TotalDokumen1 halamanDRIVE PROGRAM (2013 - 2014) : Total Total Total TotalkurutalaBelum ada peringkat
- Program Name Division Name Date Duration of Days TimeDokumen2 halamanProgram Name Division Name Date Duration of Days TimekurutalaBelum ada peringkat
- TOUCH Untrained Status (January 2014)Dokumen2 halamanTOUCH Untrained Status (January 2014)kurutalaBelum ada peringkat
- Healtheon DetailingDokumen1 halamanHealtheon DetailingkurutalaBelum ada peringkat
- La Shield DetailingDokumen2 halamanLa Shield DetailingkurutalaBelum ada peringkat
- Ascoril Expectorant - Detailing Story InterviewsDokumen2 halamanAscoril Expectorant - Detailing Story InterviewskurutalaBelum ada peringkat
- Activity Report & Monthly Planner - Training Manager - April MayDokumen4 halamanActivity Report & Monthly Planner - Training Manager - April MaykurutalaBelum ada peringkat
- SR No Division Brand: Division Wise Brands For Interview PanelDokumen1 halamanSR No Division Brand: Division Wise Brands For Interview PanelkurutalaBelum ada peringkat
- Esoz - Detailing TalkDokumen2 halamanEsoz - Detailing TalkkurutalaBelum ada peringkat
- CTV DetailingDokumen1 halamanCTV DetailingkurutalaBelum ada peringkat
- Glenmark CV DetailingDokumen1 halamanGlenmark CV DetailingkurutalaBelum ada peringkat
- Activity Report & Monthly Planner - Training Manager - AUGUST'12Dokumen4 halamanActivity Report & Monthly Planner - Training Manager - AUGUST'12kurutalaBelum ada peringkat
- The HOPE Study: (Heart Outcomes Prevention Evaluation Trial)Dokumen4 halamanThe HOPE Study: (Heart Outcomes Prevention Evaluation Trial)kurutalaBelum ada peringkat
- Critica VAF Detailing TalkDokumen1 halamanCritica VAF Detailing TalkkurutalaBelum ada peringkat
- Yearly Calender CDG ' 12-13 FinalDokumen6 halamanYearly Calender CDG ' 12-13 FinalkurutalaBelum ada peringkat
- Name of Employee Date of Birth (DD-MM-Yyyy) Contact NumberDokumen3 halamanName of Employee Date of Birth (DD-MM-Yyyy) Contact NumberkurutalaBelum ada peringkat
- 08 Drug ProfileDokumen2 halaman08 Drug ProfilekurutalaBelum ada peringkat
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- PANR Part 1Dokumen2 halamanPANR Part 1Jastine SabornidoBelum ada peringkat
- Self Assessment Guide Pharmacy Services NC IIIDokumen6 halamanSelf Assessment Guide Pharmacy Services NC IIIAnesa TuñacaoBelum ada peringkat
- Books For Mrcog Part1Dokumen2 halamanBooks For Mrcog Part1srini100% (3)
- RRQRQ: 3ttgffihrr National Medical Medical EducationDokumen2 halamanRRQRQ: 3ttgffihrr National Medical Medical EducationF LalramluahpuiaBelum ada peringkat
- Nurse ResumesDokumen4 halamanNurse ResumesPrincess Aira Bucag CarbonelBelum ada peringkat
- Jurnal B.inggris Kanker Prostat PDFDokumen17 halamanJurnal B.inggris Kanker Prostat PDFBoni Mohammad SalehBelum ada peringkat
- Proc Edur e 5 4 3 2 1: Prenatal Check-UpDokumen60 halamanProc Edur e 5 4 3 2 1: Prenatal Check-UpCharlie DyBelum ada peringkat
- Myers CocktailDokumen15 halamanMyers CocktailViladosgirassois Couto PinonBelum ada peringkat
- Group 1 Research StemDokumen55 halamanGroup 1 Research StemMary AtilloBelum ada peringkat
- WPBA HandbookDokumen261 halamanWPBA HandbookKunal MungurBelum ada peringkat
- Breastfeeding TPDokumen3 halamanBreastfeeding TPAndrea Mae SanchezBelum ada peringkat
- Brushing Teeth and RecessionDokumen16 halamanBrushing Teeth and RecessionWayan SubadiBelum ada peringkat
- Joyce Travelbee (1926 Human Relationship ModelDokumen4 halamanJoyce Travelbee (1926 Human Relationship ModelHugMoco Moco Locah ÜBelum ada peringkat
- KL Sehume Research Dissertation CDDokumen79 halamanKL Sehume Research Dissertation CDTamba KendemaBelum ada peringkat
- Par Format For Physiotherapy of NHM OdishaDokumen7 halamanPar Format For Physiotherapy of NHM Odishakrishna bptBelum ada peringkat
- Call To Action On NCDS: Challenges and Way Forward For Maternal and Child HealthDokumen32 halamanCall To Action On NCDS: Challenges and Way Forward For Maternal and Child HealthSadi KhanBelum ada peringkat
- HidrosefalusDokumen13 halamanHidrosefalusmelvinia.savitri19Belum ada peringkat
- COPD Case PresentationDokumen15 halamanCOPD Case PresentationBola Kwentua29% (7)
- BCS Guidance On Workload For Cardiologists - Final March 2010Dokumen9 halamanBCS Guidance On Workload For Cardiologists - Final March 2010Narendra KumarBelum ada peringkat
- Hrsa Sbss Hshs 041921Dokumen46 halamanHrsa Sbss Hshs 041921Donald WheelerBelum ada peringkat
- SynopsisDokumen5 halamanSynopsiskashyap kasminBelum ada peringkat
- Delivery of Health Care Services in RuralDokumen29 halamanDelivery of Health Care Services in RuralMahenurBelum ada peringkat
- M E W S: Mews (Odified Arly Arning Ystem) 3 2 1 0 1 2 3 ScoreDokumen1 halamanM E W S: Mews (Odified Arly Arning Ystem) 3 2 1 0 1 2 3 ScoreMimi SunaryantiBelum ada peringkat
- High Risk PregnanciesDokumen27 halamanHigh Risk PregnanciesMochammad Adam EldiBelum ada peringkat
- Proton Beam TherapyDokumen34 halamanProton Beam Therapyyee siew huatBelum ada peringkat
- HIV - Aids Lecture DR Nabil.1Dokumen25 halamanHIV - Aids Lecture DR Nabil.1Hannan AliBelum ada peringkat
- Martindale The Complete Drug Reference 38th Edition Free Download PDFDokumen3 halamanMartindale The Complete Drug Reference 38th Edition Free Download PDFChristian SosaBelum ada peringkat
- Unit 2A - Course NotesDokumen162 halamanUnit 2A - Course Notesrashid zaman100% (5)
- Running Head: Social Media and The Modern Impact of Informatics 1Dokumen3 halamanRunning Head: Social Media and The Modern Impact of Informatics 1danielBelum ada peringkat
- Acute PancreatitisDokumen7 halamanAcute PancreatitisVytheeshwaran Vedagiri100% (9)