Anda mungkin juga menyukai
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Brosur Penyuluhan Gizi Anak SekolahDokumen2 halamanBrosur Penyuluhan Gizi Anak SekolahTia AriantiBelum ada peringkat
- Jurnal 1Dokumen13 halamanJurnal 1Tia AriantiBelum ada peringkat
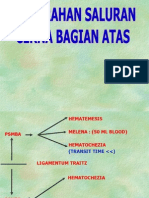
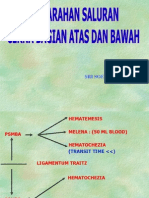
- Perdarahan Saluran Cerna Atas Dan BawahDokumen24 halamanPerdarahan Saluran Cerna Atas Dan BawahTia AriantiBelum ada peringkat
- Penyakit Jantung HipertensiDokumen24 halamanPenyakit Jantung HipertensiTia AriantiBelum ada peringkat
- Soal Ujian EkgDokumen12 halamanSoal Ujian EkgTia AriantiBelum ada peringkat
- Fatty Liver - HandoutDokumen31 halamanFatty Liver - HandoutTia AriantiBelum ada peringkat
- Chapter 9 Urinary System: Lesson 1Dokumen23 halamanChapter 9 Urinary System: Lesson 1Tia AriantiBelum ada peringkat
- Congestive Heart Failure CHF: Nik Nikam, M.DDokumen94 halamanCongestive Heart Failure CHF: Nik Nikam, M.DTia AriantiBelum ada peringkat
- Perdarahan Saluran Cerna Atas Dan BawahDokumen34 halamanPerdarahan Saluran Cerna Atas Dan BawahTia AriantiBelum ada peringkat
- Art and Science of UrinalysisDokumen31 halamanArt and Science of UrinalysisTia AriantiBelum ada peringkat
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- 04.practice Set SSC-CGL TIER I PDFDokumen16 halaman04.practice Set SSC-CGL TIER I PDFmanuBelum ada peringkat
- Assessment of The Peripheral Vascular SystemDokumen3 halamanAssessment of The Peripheral Vascular SystemTrisha Andrea DavaBelum ada peringkat
- Anatomy Physiology Exam QuestionsDokumen160 halamanAnatomy Physiology Exam Questionssyafi zulBelum ada peringkat
- Edexcel International A Levels Biology Unit 1 Wbi11 PDFDokumen18 halamanEdexcel International A Levels Biology Unit 1 Wbi11 PDFtas xo100% (1)
- Compositae FamilyDokumen23 halamanCompositae FamilyA.H. Lammert Holdijk100% (1)
- 2000 Bookmatter TextbookOfAngiologyDokumen19 halaman2000 Bookmatter TextbookOfAngiologydavidmarkovic032Belum ada peringkat
- Keith R Poskitt - Chronic Ulceration of The LegDokumen5 halamanKeith R Poskitt - Chronic Ulceration of The LegKovoor LedchumananBelum ada peringkat
- Italian Doctors, Found That It Is NOT A VIRUS But A BACTERIA That Causes Death.Dokumen3 halamanItalian Doctors, Found That It Is NOT A VIRUS But A BACTERIA That Causes Death.tesla2008Belum ada peringkat
- Blood CirculationDokumen42 halamanBlood CirculationAshu kumar100% (1)
- Central Venous Access - 2019 (Gen, Ind-Contr)Dokumen6 halamanCentral Venous Access - 2019 (Gen, Ind-Contr)Carlos NoronaBelum ada peringkat
- Hypertension CaseDokumen3 halamanHypertension CaseArnold Christian QuilonBelum ada peringkat
- Learning Guide: Central Texas College Department of NursingDokumen26 halamanLearning Guide: Central Texas College Department of Nursingapi-3697326Belum ada peringkat
- AQA Biology Seperate Science (Unit3) Summary NotesDokumen28 halamanAQA Biology Seperate Science (Unit3) Summary NotesKeval VaghjianiBelum ada peringkat
- Anatomy of The Upper Limb - Blood VesselsDokumen35 halamanAnatomy of The Upper Limb - Blood VesselsMel SionzonBelum ada peringkat
- An Scie Report Final1Dokumen5 halamanAn Scie Report Final1Abas S. AcmadBelum ada peringkat
- Cardiovascular Study GuideDokumen19 halamanCardiovascular Study GuideLouise FraserBelum ada peringkat
- Venous Lakes of The Face 253Dokumen1 halamanVenous Lakes of The Face 253Medtext PublicationsBelum ada peringkat
- Cardio NclexDokumen40 halamanCardio NclexGabrielle WashingtonBelum ada peringkat
- COVID19 Clinical Education Venous Access Comparison GuideDokumen3 halamanCOVID19 Clinical Education Venous Access Comparison Guidemew2xxBelum ada peringkat
- Sulfur Cures 2000Dokumen34 halamanSulfur Cures 2000ocoxodoBelum ada peringkat
- Our Incredible Human Body MachineDokumen44 halamanOur Incredible Human Body MachinePusat Bahasa BandungBelum ada peringkat
- Anatomy & Physiology QuestionsDokumen10 halamanAnatomy & Physiology Questionskrishna chandrakani100% (2)
- A&p (B&C) Handout 2015Dokumen50 halamanA&p (B&C) Handout 2015Alisa BrownBelum ada peringkat
- Inspired by Nature:Jan 2018 PDFDokumen117 halamanInspired by Nature:Jan 2018 PDFAkshaya Kumar Rath100% (2)
- RT 312 Prelim NotesDokumen20 halamanRT 312 Prelim NotesGiralph NikkoBelum ada peringkat
- Chapter 74Dokumen4 halamanChapter 74Regina Ysabel SartagudaBelum ada peringkat
- Full Download Ebook PDF Human Biology Concepts and Current Issues 8th Edition PDFDokumen41 halamanFull Download Ebook PDF Human Biology Concepts and Current Issues 8th Edition PDFwilliam.decosta187100% (37)
- Written Report Copy BloodDokumen29 halamanWritten Report Copy BloodNathalieCaracaBelum ada peringkat
- Demo - Lesson Plan. TetDokumen10 halamanDemo - Lesson Plan. TetGen MendozaBelum ada peringkat
- Heart Failure 2011 SVDokumen74 halamanHeart Failure 2011 SVtoobstudyingBelum ada peringkat