Anda mungkin juga menyukai
- Drug InteractionDokumen24 halamanDrug InteractionChuol Mateat KanBelum ada peringkat
- Adverse Drug Reaction - FinaleDokumen67 halamanAdverse Drug Reaction - FinaleMiguel Ligas0% (1)
- Pharmaco DynamicsDokumen34 halamanPharmaco DynamicsDrMohan GuptaBelum ada peringkat
- Fundamental Concepts of PharmacologyDokumen21 halamanFundamental Concepts of PharmacologyYean Delos ReyesBelum ada peringkat
- Amien GPP 6 MedDokumen25 halamanAmien GPP 6 MedAmanuel MaruBelum ada peringkat
- Pharmacology Review: Characteristics of DrugsDokumen11 halamanPharmacology Review: Characteristics of DrugsPaige Heath ButlerBelum ada peringkat
- Factors Modifying Drug EffectDokumen43 halamanFactors Modifying Drug EffectSunil100% (4)
- Pos OlogyDokumen25 halamanPos OlogyMonica MuruganBelum ada peringkat
- Drug Interaction:: Age, GeneticsDokumen87 halamanDrug Interaction:: Age, GeneticsMiranda MetriaBelum ada peringkat
- Drug Ons: AdverseDokumen5 halamanDrug Ons: AdverseMisty CheifBelum ada peringkat
- 1 Drug Interaction Spring 2024Dokumen68 halaman1 Drug Interaction Spring 2024192315Belum ada peringkat
- Posology Notes Yuppie's GaloreDokumen6 halamanPosology Notes Yuppie's GaloreYuppie RajBelum ada peringkat
- Factors Affecting Drug ResponseDokumen27 halamanFactors Affecting Drug ResponsehusshamBelum ada peringkat
- Factors Modifying Action of DrugsDokumen28 halamanFactors Modifying Action of DrugsGetom NgukirBelum ada peringkat
- Farmakodinamika Ii 2018Dokumen47 halamanFarmakodinamika Ii 2018PranalosaBelum ada peringkat
- Adr NewDokumen43 halamanAdr Newshyamsundermaurya987Belum ada peringkat
- Student Handout Part 2Dokumen9 halamanStudent Handout Part 2Mikaella EnriquezBelum ada peringkat
- Assignment PharmaDokumen10 halamanAssignment Pharmac2bmqsfkp7Belum ada peringkat
- Handbook of Drug Interaction and the Mechanism of InteractionDari EverandHandbook of Drug Interaction and the Mechanism of InteractionPenilaian: 1 dari 5 bintang1/5 (1)
- Pharmacodyanamics-Model Questions & AnswersDokumen6 halamanPharmacodyanamics-Model Questions & AnswersDr.U.P.Rathnakar.MD.DIH.PGDHMBelum ada peringkat
- PharmacologyDokumen52 halamanPharmacologyKris Ann Yap-BonillaBelum ada peringkat
- Pharamacodynamics Dentistry International Shahinaz Shalaby 2018Dokumen52 halamanPharamacodynamics Dentistry International Shahinaz Shalaby 2018Shahinaz ShamsBelum ada peringkat
- Adverse Drug Reactions NotesDokumen4 halamanAdverse Drug Reactions NoteskarthikeyanpgtBelum ada peringkat
- PHARMACODYNAMICSDokumen62 halamanPHARMACODYNAMICSJulius Kent QuilapioBelum ada peringkat
- 1 - Introduction To PharmacologyDokumen31 halaman1 - Introduction To PharmacologyTanvir FahimBelum ada peringkat
- Pharmacodynamics: BIOL 122 DR Hemant MehtaDokumen13 halamanPharmacodynamics: BIOL 122 DR Hemant MehtaRavinder KaurBelum ada peringkat
- Pharmaco Vig Gi LanceDokumen34 halamanPharmaco Vig Gi Lancebagir_dm10Belum ada peringkat
- Introduction To Pharmacology: Definition of TermsDokumen4 halamanIntroduction To Pharmacology: Definition of Termsdemenace1956Belum ada peringkat
- Saftey Margin & Drug ToxicityDokumen27 halamanSaftey Margin & Drug Toxicitysubhashish01Belum ada peringkat
- Medications: Prepared By: Aleli R. Cheng, RN, MANDokumen128 halamanMedications: Prepared By: Aleli R. Cheng, RN, MANalelichengBelum ada peringkat
- NMPHHN280 Module4Dokumen49 halamanNMPHHN280 Module4강소라Belum ada peringkat
- Factors Modifying Drug ActionsDokumen3 halamanFactors Modifying Drug ActionsDAMBALE0% (1)
- Fundamentals of Pharmcology: Nursing Facts in BriefDokumen4 halamanFundamentals of Pharmcology: Nursing Facts in Briefanne009Belum ada peringkat
- Ilovepdf Merged PDFDokumen705 halamanIlovepdf Merged PDFAli MohammedBelum ada peringkat
- Adverse Drug ReactionDokumen108 halamanAdverse Drug ReactionBinod Sah100% (2)
- 01.EMMS - General Pharmacology 1Dokumen32 halaman01.EMMS - General Pharmacology 1Faisal FahadBelum ada peringkat
- Factors Modifying The Drug ActionDokumen6 halamanFactors Modifying The Drug ActionNil GyiBelum ada peringkat
- A Presentation On Adr Due To AntibioitcsDokumen18 halamanA Presentation On Adr Due To AntibioitcsAnta SharmaBelum ada peringkat
- Adverse Drug ReactionDokumen6 halamanAdverse Drug ReactionNunkoo RajBelum ada peringkat
- Adverse Drug ReactionDokumen6 halamanAdverse Drug Reactionpranal patil (Pranal)Belum ada peringkat
- Adverse EffectsDokumen27 halamanAdverse EffectsNoha AzzamBelum ada peringkat
- Chapter 1 - Introduction To PharmacologyDokumen35 halamanChapter 1 - Introduction To Pharmacologyjungemica0214Belum ada peringkat
- Pengantar Interaksi Obat: Drug InteractionDokumen21 halamanPengantar Interaksi Obat: Drug InteractionFaykar RezaBelum ada peringkat
- ADR Final1Dokumen10 halamanADR Final1Rubina BisankheBelum ada peringkat
- N-Lec3 - PharmacotherapeuticsDokumen29 halamanN-Lec3 - Pharmacotherapeuticsgeng gengBelum ada peringkat
- Drug Chemical Name Generic Name Trade Name Drug Classification PharmaceuticsDokumen5 halamanDrug Chemical Name Generic Name Trade Name Drug Classification Pharmaceuticschubbygunny_29776413Belum ada peringkat
- Drug Interaction Can Be Defined As TheDokumen34 halamanDrug Interaction Can Be Defined As TheIstianah Es100% (1)
- 7.factors Modifying Drug ActionDokumen36 halaman7.factors Modifying Drug ActionOsama KhanBelum ada peringkat
- ADR Notes KINJAL S. GAMITDokumen13 halamanADR Notes KINJAL S. GAMITKinjal GamitBelum ada peringkat
- 2018 Obat Pada ManulaDokumen62 halaman2018 Obat Pada ManulaShafira Nur Amalia ZulvaBelum ada peringkat
- PharmacodynamicsDokumen50 halamanPharmacodynamicsRochelle RagoBelum ada peringkat
- NCM105 13th PsychopharmacologyDokumen17 halamanNCM105 13th PsychopharmacologyKamx MohammedBelum ada peringkat
- ADR Reaction, Medication Error and Drug InteractionDokumen86 halamanADR Reaction, Medication Error and Drug Interactionada atienzaBelum ada peringkat
- Drug InteractionDokumen26 halamanDrug InteractionABDURRAHMAN ASY-SYAKUUR 1Belum ada peringkat
- Digestive System Diseases and Therapy NotesDokumen19 halamanDigestive System Diseases and Therapy NotesMbah GapinbissiBelum ada peringkat
- Adr and ManagementDokumen48 halamanAdr and ManagementDhanush G V DhanushBelum ada peringkat
- Adverse Drug ReactionsDokumen64 halamanAdverse Drug ReactionsSunanda mohanBelum ada peringkat
- ADRsDokumen56 halamanADRsFarina FaraziBelum ada peringkat
- Autonomic Nervous System & Homeopathy: Personalized Nutrition Concept Depicted in Homeopathy & AyurvedaDari EverandAutonomic Nervous System & Homeopathy: Personalized Nutrition Concept Depicted in Homeopathy & AyurvedaBelum ada peringkat
- MetronidazoleDokumen2 halamanMetronidazoleGwyn RosalesBelum ada peringkat
- Ven List 2015 Jamaica 2015Dokumen57 halamanVen List 2015 Jamaica 2015Aulia KpBelum ada peringkat
- Medic Amen ToDokumen115 halamanMedic Amen ToErik FerreiraBelum ada peringkat
- Characteristics of MetamizoleDokumen9 halamanCharacteristics of MetamizoleLisa NPBelum ada peringkat
- Contract Research Organizations An Industry AnalysisDokumen25 halamanContract Research Organizations An Industry AnalysisJürgen FleischerBelum ada peringkat
- Solubility and PermeabilityDokumen3 halamanSolubility and PermeabilityGNCDWBelum ada peringkat
- Physostigmine - ClinicalKeyDokumen11 halamanPhysostigmine - ClinicalKeyHenry Leroy Lewis BatresBelum ada peringkat
- AdvairDokumen1 halamanAdvairE50% (2)
- NARITADokumen14 halamanNARITASYAFAA FARMABelum ada peringkat
- The British Journal of Cardiology May-June 2010, Volume 17 Supplement 2Dokumen16 halamanThe British Journal of Cardiology May-June 2010, Volume 17 Supplement 2mbarrales_4Belum ada peringkat
- Resep (Disalin Sesuai Aslinya) Drug Related Problem (S) : Kertas Kerja Tinjauan Dan Pelayanan ResepDokumen3 halamanResep (Disalin Sesuai Aslinya) Drug Related Problem (S) : Kertas Kerja Tinjauan Dan Pelayanan ResepHerlina AlfianyBelum ada peringkat
- Even 1st Mid - Sem - Schedule - Final 2022-23Dokumen50 halamanEven 1st Mid - Sem - Schedule - Final 2022-23lingu easyBelum ada peringkat
- A Large Prospective Open-Label Multicent PDFDokumen6 halamanA Large Prospective Open-Label Multicent PDFsyeda tahsin naharBelum ada peringkat
- Computational Models For Drug Design and DelivDokumen235 halamanComputational Models For Drug Design and DelivIbrahim Al SharabiBelum ada peringkat
- Fexofenadine Hydro ChlorideDokumen2 halamanFexofenadine Hydro Chlorideapi-3797941Belum ada peringkat
- CM-1092-01 - Module 01Dokumen76 halamanCM-1092-01 - Module 01Hoa Linh GMPBelum ada peringkat
- ClotrimazoleDokumen2 halamanClotrimazoleSagar GuptaBelum ada peringkat
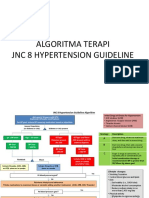
- 2 Algoritma HT JNC 8Dokumen3 halaman2 Algoritma HT JNC 8Nais Maghfiroh100% (1)
- Item 2 Reading ListDokumen3 halamanItem 2 Reading Listksrinu9988Belum ada peringkat
- Drugs Society and Human Behavior 16th Edition Hart Test BankDokumen12 halamanDrugs Society and Human Behavior 16th Edition Hart Test Bankmichelleortizpxnzkycmbw100% (28)
- Guideline For Field Visit ReportDokumen4 halamanGuideline For Field Visit Reportmdkasim904Belum ada peringkat
- Microbial ResistanceDokumen16 halamanMicrobial ResistanceDixa MeBelum ada peringkat
- Stock Dma 27 Juli 20Dokumen1.918 halamanStock Dma 27 Juli 20Rila Vita SariBelum ada peringkat
- SedativesDokumen4 halamanSedativesalghashm001Belum ada peringkat
- Antihistamines General StatementDokumen68 halamanAntihistamines General StatementJuniver Verriansyach PakajaBelum ada peringkat
- Rekap HargaDokumen72 halamanRekap HargaGani Hyman ShahihBelum ada peringkat
- Report No: MSE/JEL/EXM/CRISP/PMI/F/001Dokumen20 halamanReport No: MSE/JEL/EXM/CRISP/PMI/F/001Thiru RajaBelum ada peringkat
- Inhalers Used in Asthma and COPD PDFDokumen1 halamanInhalers Used in Asthma and COPD PDFconBelum ada peringkat
- Desloratadine - A New, Nonsedating, Oral AntihistamineDokumen12 halamanDesloratadine - A New, Nonsedating, Oral AntihistamineAnonymous so6ZnlKywBelum ada peringkat
- Industrial Training Performed at Piramal Pharma Solutions, Mahad, Dist-RaigadDokumen32 halamanIndustrial Training Performed at Piramal Pharma Solutions, Mahad, Dist-RaigadChandan A. Wagh100% (1)