Anda mungkin juga menyukai
- Condensesure BrochureDokumen6 halamanCondensesure Brochureloulou612Belum ada peringkat
- Worcester Greenstar System Filter BrochureDokumen6 halamanWorcester Greenstar System Filter Brochureloulou612Belum ada peringkat
- Greenstar Gas Boilers BrochureDokumen36 halamanGreenstar Gas Boilers Brochureloulou612Belum ada peringkat
- Family DynamicsDokumen5 halamanFamily Dynamicsloulou612Belum ada peringkat
- Integral Charging Link Fitting and User InstructionsDokumen4 halamanIntegral Charging Link Fitting and User Instructionsloulou612Belum ada peringkat
- Homeostasis PresentationDokumen16 halamanHomeostasis Presentationloulou612100% (1)
- DPS Personal Hygiene and Oral CareDokumen17 halamanDPS Personal Hygiene and Oral Careloulou612Belum ada peringkat
- Skin 2012Dokumen21 halamanSkin 2012loulou612Belum ada peringkat
- Thermoregulation 2012Dokumen17 halamanThermoregulation 2012loulou612Belum ada peringkat
- The Cell Student Copy 2012Dokumen29 halamanThe Cell Student Copy 2012loulou612Belum ada peringkat
- EU Foreign Policy - Key Developments and Controversies.: Palestine KabulDokumen10 halamanEU Foreign Policy - Key Developments and Controversies.: Palestine Kabulloulou612Belum ada peringkat
- Care Stands For: C A R E: WWW - Thecarecampaign.co - UkDokumen1 halamanCare Stands For: C A R E: WWW - Thecarecampaign.co - Ukloulou612Belum ada peringkat
- The European Commission: - Structure - Tasks - Powers - ProblemsDokumen14 halamanThe European Commission: - Structure - Tasks - Powers - Problemsloulou612Belum ada peringkat
- Ethnicity and InequalityDokumen16 halamanEthnicity and Inequalityloulou612Belum ada peringkat
- The Impact of CAP Reform: Dr. Franz FISCHLERDokumen17 halamanThe Impact of CAP Reform: Dr. Franz FISCHLERloulou612Belum ada peringkat
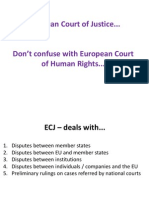
- ECJ Overview 2012v2Dokumen10 halamanECJ Overview 2012v2loulou612Belum ada peringkat
- Biodiversity and Climate ChangeDokumen7 halamanBiodiversity and Climate Changeloulou612Belum ada peringkat
- Effectiveness of LordsDokumen1 halamanEffectiveness of Lordsloulou612Belum ada peringkat
- UK Pressure Groups - How They Exert Influence Across The EUDokumen33 halamanUK Pressure Groups - How They Exert Influence Across The EUloulou612Belum ada peringkat
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Westwood Community v. John P. Barbee, 293 F.3d 1332, 11th Cir. (2002)Dokumen8 halamanWestwood Community v. John P. Barbee, 293 F.3d 1332, 11th Cir. (2002)Scribd Government DocsBelum ada peringkat
- Davao Smoking LawDokumen4 halamanDavao Smoking LawJohn Remy HerbitoBelum ada peringkat
- Crimpro Case DoctrinesDokumen39 halamanCrimpro Case DoctrinesAleezah Gertrude RaymundoBelum ada peringkat
- Intestate Estate of Don Mariano San Pedro v. Court of Appeals, GR No. 103727, Dec. 1, 1996Dokumen3 halamanIntestate Estate of Don Mariano San Pedro v. Court of Appeals, GR No. 103727, Dec. 1, 1996Jamiah Obillo HulipasBelum ada peringkat
- Lecture 4 - 6 - Law of ContractDokumen20 halamanLecture 4 - 6 - Law of ContractSrezon HalderBelum ada peringkat
- Defensor-Santiago v. SandiganbayanDokumen3 halamanDefensor-Santiago v. SandiganbayanDaryl YuBelum ada peringkat
- Ra 7470 Ra 349Dokumen5 halamanRa 7470 Ra 349Lee Anne Santos - JavierBelum ada peringkat
- McFarland VDokumen2 halamanMcFarland Vhypertxi1Belum ada peringkat
- Law of Crime (Indian Pinal Code) - I594 - Xid-3956263 - 1Dokumen2 halamanLaw of Crime (Indian Pinal Code) - I594 - Xid-3956263 - 1Nidhi HiranwarBelum ada peringkat
- Icc A 2009Dokumen3 halamanIcc A 2009Sana KhairiBelum ada peringkat
- Annex C - APOR Affidavit of UndertakingDokumen1 halamanAnnex C - APOR Affidavit of UndertakingAlex JayBelum ada peringkat
- NAFLU V OpleDokumen3 halamanNAFLU V OpleAnit EmersonBelum ada peringkat
- Extended Response (Electroral College)Dokumen2 halamanExtended Response (Electroral College)htarhtar28011Belum ada peringkat
- Eduarte vs. Court of Appeals, 253 SCRA 391, February 09, 1996Dokumen15 halamanEduarte vs. Court of Appeals, 253 SCRA 391, February 09, 1996Kath OBelum ada peringkat
- Eric Young v. Jodi Blatt, 4th Cir. (2014)Dokumen2 halamanEric Young v. Jodi Blatt, 4th Cir. (2014)Scribd Government DocsBelum ada peringkat
- San Juan de Dios v. NLRC (Case Digest)Dokumen2 halamanSan Juan de Dios v. NLRC (Case Digest)Czarina Louise NavarroBelum ada peringkat
- The Rise of Extra-Legal RemediesDokumen3 halamanThe Rise of Extra-Legal Remediesem corderoBelum ada peringkat
- Kyc PDFDokumen9 halamanKyc PDFOnn InternationalBelum ada peringkat
- Application EnrolmentDokumen5 halamanApplication EnrolmentBbaale AdvocatesBelum ada peringkat
- Section 6. - Right To Choose Abode & Right To Travel at Home & Out of CountryDokumen19 halamanSection 6. - Right To Choose Abode & Right To Travel at Home & Out of CountryANDREA JOSES TANBelum ada peringkat
- CSIS Injury AssessmentDokumen8 halamanCSIS Injury Assessmentthe fifth estateBelum ada peringkat
- Metropolitan Bank V GonzalesDokumen1 halamanMetropolitan Bank V GonzalesYasuhiro Kei100% (1)
- Final Exam Tax2 With AnswersDokumen6 halamanFinal Exam Tax2 With AnswersNikki Estores GonzalesBelum ada peringkat
- Cdi4 W7Dokumen4 halamanCdi4 W7ALBANIEL, ANDREA CLARISSE C.Belum ada peringkat
- Cape Coral Mowing OrdinanceDokumen5 halamanCape Coral Mowing OrdinanceNews-PressBelum ada peringkat
- Bar Council of India Powers and FunctionsDokumen11 halamanBar Council of India Powers and FunctionsSonu Pandit100% (1)
- Johor Coastal Development SDN BHD V Constrajaya SDN BHDDokumen17 halamanJohor Coastal Development SDN BHD V Constrajaya SDN BHDYumiko HoBelum ada peringkat
- Mindanao Development Authority V CADokumen11 halamanMindanao Development Authority V CARubyBelum ada peringkat
- Coronado vs. CADokumen5 halamanCoronado vs. CAashaxleBelum ada peringkat
- Republic Act No. 10368 - Official Gazette of The Republic of The PhilippinesDokumen14 halamanRepublic Act No. 10368 - Official Gazette of The Republic of The PhilippinesJay Dimakuta MacarambonBelum ada peringkat