Anda mungkin juga menyukai
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5782)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (72)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Progress Report-4Dokumen20 halamanProgress Report-4api-613937515Belum ada peringkat
- Thrive Strongman ProgramDokumen6 halamanThrive Strongman Programahmed z falahBelum ada peringkat
- GeographyDokumen4 halamanGeographyNol TasholliBelum ada peringkat
- Math 3Eng-T Engineering Data Analysis Problem Set #4 Due Date: Sep 24, 2020 (12 NN) Justin M. Marquez BET-Automotive General InstructionsDokumen5 halamanMath 3Eng-T Engineering Data Analysis Problem Set #4 Due Date: Sep 24, 2020 (12 NN) Justin M. Marquez BET-Automotive General InstructionsDeniell Joyce MarquezBelum ada peringkat
- Howells, J., & Bessant, J. (2012) - Introduction Innovation and Economic Geography A Review and AnalysisDokumen14 halamanHowells, J., & Bessant, J. (2012) - Introduction Innovation and Economic Geography A Review and AnalysisafafsdfsdgsdBelum ada peringkat
- Art07 EngDokumen8 halamanArt07 Engcerbu_bass_cdcBelum ada peringkat
- Compact and Medium Hammer BrochureDokumen12 halamanCompact and Medium Hammer BrochureMMM-MMMBelum ada peringkat
- JEE 2023 Session-1 24th Jan To 1st Feb 2023Dokumen37 halamanJEE 2023 Session-1 24th Jan To 1st Feb 2023Harshith Reddy GantaBelum ada peringkat
- Napco XP-600 User Guide (Leon Terrace)Dokumen16 halamanNapco XP-600 User Guide (Leon Terrace)Malcolm KeevyBelum ada peringkat
- Lab 1 - Diode Characteristics and ApplicationsDokumen8 halamanLab 1 - Diode Characteristics and ApplicationsMD NAZMUN HASAN NAFEESBelum ada peringkat
- Concrete Technology, Basics of ConcreteDokumen80 halamanConcrete Technology, Basics of ConcreteAhsan Rabbani100% (3)
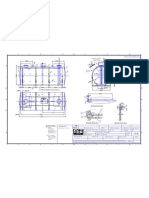
- Saddle Positioning (500m3)Dokumen1 halamanSaddle Positioning (500m3)solquihaBelum ada peringkat
- Semperit Databook en PDFDokumen22 halamanSemperit Databook en PDFColhiisBelum ada peringkat
- Micro Cold Storage: Ecozen SolutionsDokumen2 halamanMicro Cold Storage: Ecozen SolutionsVikram DeshmukhBelum ada peringkat
- Fluid and Electrolyte Balance: Presenter: Dr. Siyum Mathewos (Omfs-Ri) Modulator: Dr. Dereje (Omfs, Consultant)Dokumen87 halamanFluid and Electrolyte Balance: Presenter: Dr. Siyum Mathewos (Omfs-Ri) Modulator: Dr. Dereje (Omfs, Consultant)Siyum MathewosBelum ada peringkat
- Ch10 LectureDokumen53 halamanCh10 LectureaikatBelum ada peringkat
- 4 X 50 W Quad Bridge Car Radio Amplifier: FeatureDokumen9 halaman4 X 50 W Quad Bridge Car Radio Amplifier: FeatureMerkar ElektronikBelum ada peringkat
- Alta Slot IntermittentDokumen51 halamanAlta Slot IntermittentHabib RajuBelum ada peringkat
- SOAL SULIT UN 2017/2018 IDENTIFIKASI DAN PEMBAHASANDokumen12 halamanSOAL SULIT UN 2017/2018 IDENTIFIKASI DAN PEMBAHASANJuzt JoBelum ada peringkat
- Introduction: Need For: MCMT Mapping Course Outcomes Woth Program OutcomesDokumen3 halamanIntroduction: Need For: MCMT Mapping Course Outcomes Woth Program OutcomesKalai ArasanBelum ada peringkat
- AminesDokumen1 halamanAminesAtul SharmaBelum ada peringkat
- Spring 2019 Journal WebDokumen28 halamanSpring 2019 Journal WebCarlos Jose Prada RangelBelum ada peringkat
- UK Portal Frame CalculationDokumen57 halamanUK Portal Frame CalculationKhairul JaggerBelum ada peringkat
- PlantLifeCycleAnchorChartsFREEBIE PDFDokumen5 halamanPlantLifeCycleAnchorChartsFREEBIE PDFAisha L'shaimy100% (1)
- Vibration Control Catalog - TechDokumen72 halamanVibration Control Catalog - TechStuart TangBelum ada peringkat
- Service Manual Sigma Air Control Plus: Article Number: 7.7740.0 7.7741.0 7.7742.0Dokumen47 halamanService Manual Sigma Air Control Plus: Article Number: 7.7740.0 7.7741.0 7.7742.0Evandro Jva compressoresBelum ada peringkat
- David Parts List and InvoiceDokumen4 halamanDavid Parts List and InvoiceM B F SOLUTIONBelum ada peringkat
- A5. Ficha Técnica S4E500AM0301Dokumen6 halamanA5. Ficha Técnica S4E500AM0301Ruben3012Belum ada peringkat
- Texas Instrument - Wireless PH Sensor TransmitterDokumen28 halamanTexas Instrument - Wireless PH Sensor Transmitterthiennd831410Belum ada peringkat
- Eating Habits in VietnamDokumen3 halamanEating Habits in Vietnamsuachuamatong2501Belum ada peringkat