Anda mungkin juga menyukai
- Anatomy, Physiology and Pathology of The RespiratoryDokumen68 halamanAnatomy, Physiology and Pathology of The Respiratorytheresia_s_k100% (1)
- Word Bank: Edward Lee Physiology Test RespDokumen11 halamanWord Bank: Edward Lee Physiology Test RespEdward LeeBelum ada peringkat
- Respiratory System Part 1Dokumen8 halamanRespiratory System Part 1brooklynBelum ada peringkat
- The Respiratory SystemDokumen37 halamanThe Respiratory SystemriverBelum ada peringkat
- Anatomy and Physiology of The Respiratory TractDokumen49 halamanAnatomy and Physiology of The Respiratory TractshvnagaBelum ada peringkat
- RespiratoryDokumen62 halamanRespiratoryDerón Asbery HolmesBelum ada peringkat
- Human Respiratory System and MechanicsDokumen105 halamanHuman Respiratory System and MechanicsAbdul Qadir100% (1)
- Respiratory System Gas ExchangeDokumen64 halamanRespiratory System Gas ExchangenashqonashBelum ada peringkat
- Respiratory System: Anatomy & PhysiologyDokumen111 halamanRespiratory System: Anatomy & PhysiologyJape GarridoBelum ada peringkat
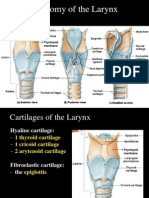
- Anatomy of The Larynx: Thyrohyoid MembraneDokumen35 halamanAnatomy of The Larynx: Thyrohyoid MembraneVarsha Shende KhobragadeBelum ada peringkat
- Lecture 5 Respiratory System 1Dokumen61 halamanLecture 5 Respiratory System 1hafiz patahBelum ada peringkat
- Respiratory A StudentDokumen16 halamanRespiratory A Student46bwilsonBelum ada peringkat
- Functions of The Respiratory SystemDokumen10 halamanFunctions of The Respiratory SystemKrisha AvorqueBelum ada peringkat
- The Respiratory System: ASTIKA NUR ROHMAH, S.Kep., NS., M.BiomedDokumen43 halamanThe Respiratory System: ASTIKA NUR ROHMAH, S.Kep., NS., M.BiomedAdek KhazeliaBelum ada peringkat
- Respiratory System Overview and Gas ExchangeDokumen64 halamanRespiratory System Overview and Gas ExchangeNabilaBelum ada peringkat
- Respiratory System PDFDokumen16 halamanRespiratory System PDFMary Ann SacramentoBelum ada peringkat
- Kuliah 3 Respirasi + CardiovasculerDokumen73 halamanKuliah 3 Respirasi + CardiovasculerNindya Alfa DichaBelum ada peringkat
- Respiratory System Functions and AnatomyDokumen40 halamanRespiratory System Functions and AnatomychromaBelum ada peringkat
- Respiratory Physiology IDokumen47 halamanRespiratory Physiology IDeea LobonțiuBelum ada peringkat
- The Respiratory System: Raymund Christopher R. Dela Peña, RN, RM, MAN Clinical Faculty UNP-College of NursingDokumen95 halamanThe Respiratory System: Raymund Christopher R. Dela Peña, RN, RM, MAN Clinical Faculty UNP-College of NursingrnrmmanphdBelum ada peringkat
- Alterations in OxygenationDokumen104 halamanAlterations in OxygenationMelchor Felipe Salvosa100% (1)
- Respiratory SystemDokumen49 halamanRespiratory SystemVishal SharmaBelum ada peringkat
- Respiratory System Handout Explains Lung Functions & AnatomyDokumen10 halamanRespiratory System Handout Explains Lung Functions & AnatomyMr. DummyBelum ada peringkat
- Anatomy & PhysiologyDokumen42 halamanAnatomy & PhysiologyArah Lyn ApiagBelum ada peringkat
- Anatomi Sistem ParuDokumen64 halamanAnatomi Sistem ParuMochammad Fariz AmsalBelum ada peringkat
- Respiratory PhysiologyDokumen39 halamanRespiratory Physiologytesfamichael mengistuBelum ada peringkat
- 1.anatomy of Respiratory SystemDokumen73 halaman1.anatomy of Respiratory Systemokoti.omutanyi22Belum ada peringkat
- Respiratory System: An Overview of Functions, Anatomy and Gas ExchangeDokumen25 halamanRespiratory System: An Overview of Functions, Anatomy and Gas ExchangeKangwa MasekaBelum ada peringkat
- Functional anatomy of pulmonary system, pulmonary circulation and mechanics of breathingDokumen98 halamanFunctional anatomy of pulmonary system, pulmonary circulation and mechanics of breathingdrusmanjamilhcmdBelum ada peringkat
- The Respiratory SystemDokumen147 halamanThe Respiratory SystemAya SobhiBelum ada peringkat
- UntitledDokumen62 halamanUntitledManaye MamuyeBelum ada peringkat
- Anatomy of Respiratory SystemDokumen57 halamanAnatomy of Respiratory SystemRyan LarsenBelum ada peringkat
- The Respiratory System: Structure and Gas ExchangeDokumen6 halamanThe Respiratory System: Structure and Gas ExchangeBethany CrawfordBelum ada peringkat
- Respiratory System & Auscultation: T HeffernanDokumen28 halamanRespiratory System & Auscultation: T Heffernanapi-19826220Belum ada peringkat
- Anatomy of Respiratory System: Dr. Dwi Rita Anggraini, MkesDokumen64 halamanAnatomy of Respiratory System: Dr. Dwi Rita Anggraini, MkesFira TasyaBelum ada peringkat
- Respira SiDokumen80 halamanRespira SiIlaJako StefanaticBelum ada peringkat
- Functions of the Respiratory SystemDokumen4 halamanFunctions of the Respiratory SystemAlliana Pauline AbanBelum ada peringkat
- Respiratory SystemDokumen56 halamanRespiratory SystemBenjo100% (2)
- ANATOMYDokumen53 halamanANATOMYJocel Mae OrtegaBelum ada peringkat
- Care of Clients with Respiratory ProblemsDokumen115 halamanCare of Clients with Respiratory ProblemsarielleortuosteBelum ada peringkat
- Anatomy and Functions of the Respiratory SystemDokumen77 halamanAnatomy and Functions of the Respiratory SystemYour Materials100% (1)
- Pain, Surgery and Oxygenation NursingDokumen7 halamanPain, Surgery and Oxygenation NursingJhoanna de ChavezBelum ada peringkat
- Respiratory System s2 2019Dokumen56 halamanRespiratory System s2 2019noviantyramadhani12Belum ada peringkat
- Anatomi Pertemuan 4Dokumen52 halamanAnatomi Pertemuan 4dimasBelum ada peringkat
- DR Zainuri - Embriologi Dan Topografi Trac RespiratoriusDokumen62 halamanDR Zainuri - Embriologi Dan Topografi Trac RespiratoriusLuna LitamiBelum ada peringkat
- Respiratory SystemDokumen32 halamanRespiratory Systemapi-202513022Belum ada peringkat
- Week 3 Respiratory SystemDokumen10 halamanWeek 3 Respiratory SystemangeliaBelum ada peringkat
- Respiratory SystemDokumen53 halamanRespiratory Systemmehakapoor29Belum ada peringkat
- OxygenationDokumen16 halamanOxygenationMandy Jamero100% (1)
- Respiratory System: Functions, Structures and DiseasesDokumen73 halamanRespiratory System: Functions, Structures and DiseasesAmafel TolentinoBelum ada peringkat
- ScienceDokumen14 halamanSciencesheanellerenzsantosBelum ada peringkat
- Handout On GAS EXCHANGEDokumen4 halamanHandout On GAS EXCHANGEEli Joshua EvangelistaBelum ada peringkat
- Chapter 8 - Respiratory SystemDokumen20 halamanChapter 8 - Respiratory Systemmnurnazri10Belum ada peringkat
- Wa0107.Dokumen177 halamanWa0107.Dikachi ExcellentBelum ada peringkat
- 12 - Respiratory PhysiologyDokumen62 halaman12 - Respiratory PhysiologyRohit K YBelum ada peringkat
- CH 13 - Respiratory SystemDokumen56 halamanCH 13 - Respiratory SystemAna Ats Yvi100% (4)
- Respiratory SystemDokumen53 halamanRespiratory SystemRotan CirebonBelum ada peringkat
- How Do Humans Breathe? Science Book Age 8 | Children's Biology BooksDari EverandHow Do Humans Breathe? Science Book Age 8 | Children's Biology BooksBelum ada peringkat
- DC Driver Manual 2015Dokumen101 halamanDC Driver Manual 2015vanderphysBelum ada peringkat
- F1-F2 frequency calculationsDokumen1 halamanF1-F2 frequency calculationsvanderphysBelum ada peringkat
- Phase-Shifted Rectified Sine WavesDokumen62 halamanPhase-Shifted Rectified Sine WavesvanderphysBelum ada peringkat
- Functions and Properties of Blood - Plasma - Blood Cell Production - Erythrocytes - Blood Types - Leukocytes - Hemostasis (Stoppage of Bleeding)Dokumen47 halamanFunctions and Properties of Blood - Plasma - Blood Cell Production - Erythrocytes - Blood Types - Leukocytes - Hemostasis (Stoppage of Bleeding)vanderphysBelum ada peringkat
- 13 Nervous TissueDokumen57 halaman13 Nervous TissuevanderphysBelum ada peringkat
- Logical FallaciesDokumen9 halamanLogical FallaciestlgreenokcBelum ada peringkat
- Sentence Variation Models ExplainedDokumen5 halamanSentence Variation Models ExplainedvanderphysBelum ada peringkat
- 20 Circulatory SystemDokumen81 halaman20 Circulatory SystemvanderphysBelum ada peringkat
- 1 Themes in A&PDokumen36 halaman1 Themes in A&PvanderphysBelum ada peringkat
- Study of Microscopic Anatomy - Only 200 Different Cells Types - Four Primary Tissue ClassesDokumen61 halamanStudy of Microscopic Anatomy - Only 200 Different Cells Types - Four Primary Tissue ClassesvanderphysBelum ada peringkat
- 29 Human DevelopmentDokumen53 halaman29 Human DevelopmentvanderphysBelum ada peringkat
- 24 Water, Electrolyte and Acid BaseDokumen48 halaman24 Water, Electrolyte and Acid BasevanderphysBelum ada peringkat
- Nucleus and Nucleic Acids - Protein Synthesis and Secretion - DNA Replication and The Cell Cycle - Chromosomes and HeredityDokumen53 halamanNucleus and Nucleic Acids - Protein Synthesis and Secretion - DNA Replication and The Cell Cycle - Chromosomes and HeredityvanderphysBelum ada peringkat
- 4 Cellular Form and FunctionDokumen80 halaman4 Cellular Form and FunctionvanderphysBelum ada peringkat
- Muscle Tissue Structure and Contraction MechanismsDokumen64 halamanMuscle Tissue Structure and Contraction MechanismsvanderphysBelum ada peringkat
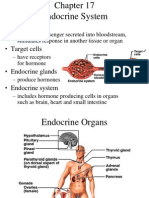
- 17 Endocrine SystemDokumen74 halaman17 Endocrine SystemvanderphysBelum ada peringkat
- 10 JointsDokumen53 halaman10 JointsvanderphysBelum ada peringkat
- 9 Skeletal SystemDokumen63 halaman9 Skeletal Systemvanderphys100% (1)
- 19 The HeartDokumen75 halaman19 The HeartvanderphysBelum ada peringkat
- Study of Microscopic Anatomy - Only 200 Different Cells Types - Four Primary Tissue ClassesDokumen61 halamanStudy of Microscopic Anatomy - Only 200 Different Cells Types - Four Primary Tissue ClassesvanderphysBelum ada peringkat
- 14 The Central Nervous SystemDokumen61 halaman14 The Central Nervous SystemvanderphysBelum ada peringkat
- 16 Sense OrgansDokumen79 halaman16 Sense OrgansvanderphysBelum ada peringkat
- Bone Tissue Structure and FunctionDokumen39 halamanBone Tissue Structure and Functionvanderphys100% (1)
- The Anatomy and Functions of the Integumentary SystemDokumen38 halamanThe Anatomy and Functions of the Integumentary Systemvanderphys100% (1)
- 25 Digestive SystemDokumen79 halaman25 Digestive SystemvanderphysBelum ada peringkat
- The Muscular System: Anatomy and FunctionsDokumen61 halamanThe Muscular System: Anatomy and FunctionsvanderphysBelum ada peringkat
- 15 PNS and ReflexesDokumen47 halaman15 PNS and Reflexesvanderphys100% (1)
- 29 Human DevelopmentDokumen53 halaman29 Human DevelopmentvanderphysBelum ada peringkat
- 25 Digestive SystemDokumen79 halaman25 Digestive SystemvanderphysBelum ada peringkat
- Test # 12 NEETPrep Test Series For NEET 2020Dokumen29 halamanTest # 12 NEETPrep Test Series For NEET 2020AXR AmstaBelum ada peringkat
- Micro Biology EMDokumen320 halamanMicro Biology EMdeliciaammuBelum ada peringkat
- Vision IAS Environment Part 1Dokumen169 halamanVision IAS Environment Part 1Anup ShindeBelum ada peringkat
- Cepheids.: No. of Systematic Area Position Variables DeviationDokumen9 halamanCepheids.: No. of Systematic Area Position Variables DeviationLefrina GusrianiiBelum ada peringkat
- Biology: University of Cambridge International Examinations General Certificate of Education Advanced LevelDokumen8 halamanBiology: University of Cambridge International Examinations General Certificate of Education Advanced LevelwegdanBelum ada peringkat
- 20-Advances in Cognitive TheoryDokumen24 halaman20-Advances in Cognitive TheoryAndrea ZeballosBelum ada peringkat
- Fertilization to Birth: A Guide to Pregnancy DevelopmentDokumen7 halamanFertilization to Birth: A Guide to Pregnancy DevelopmentSamson BongsiwBelum ada peringkat
- Chem 160.1 Post LabDokumen7 halamanChem 160.1 Post LabMarlyn AmanteBelum ada peringkat
- Rabbit Farming Business Plan PDFDokumen78 halamanRabbit Farming Business Plan PDFson82% (11)
- Tissue processing problems and artifactsDokumen18 halamanTissue processing problems and artifactsOsama Bakheet100% (2)
- Proximate Composition of Whey From South West Nigeria: Research ArticleDokumen3 halamanProximate Composition of Whey From South West Nigeria: Research Articlemilan poudelBelum ada peringkat
- Misof Et Al 2014Dokumen6 halamanMisof Et Al 2014Grant Adams100% (1)
- Mothership Character SheetDokumen2 halamanMothership Character SheetAlexander Dalton0% (1)
- WasteDokumen49 halamanWasteMirza ShahrezaBelum ada peringkat
- SPEXSP Handbook2016Dokumen126 halamanSPEXSP Handbook2016dchyBelum ada peringkat
- I. Use of English (3.0 PTS) Part A: Choose The Correct Answer To Fill in The Blank. (1.5 PTS)Dokumen6 halamanI. Use of English (3.0 PTS) Part A: Choose The Correct Answer To Fill in The Blank. (1.5 PTS)Rebecca DBelum ada peringkat
- DissertationDokumen7 halamanDissertationChandra SekharBelum ada peringkat
- Understanding Morphology Second EditionDokumen14 halamanUnderstanding Morphology Second EditionJulia TamBelum ada peringkat
- Crossword Puzzles ScienceDokumen4 halamanCrossword Puzzles ScienceNorazah AhmadBelum ada peringkat
- Digestion and AbsorptionDokumen38 halamanDigestion and Absorptionapi-226664928Belum ada peringkat
- 8.5 Power Notes PDFDokumen1 halaman8.5 Power Notes PDFMaria Jose SantamariaBelum ada peringkat
- Four New Species of RasboraDokumen25 halamanFour New Species of RasboraSubhadra LaimayumBelum ada peringkat
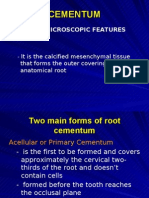
- 4 Cementum and Alveolar BoneDokumen24 halaman4 Cementum and Alveolar Boneceudmd3d100% (1)
- QTPPDokumen3 halamanQTPPRajesh Bhapkar100% (1)
- Nervous CoordinationDokumen36 halamanNervous CoordinationOlamide AyindeBelum ada peringkat
- Agroforestry As A Means of Alleviating Poverty in Sri LankaDokumen7 halamanAgroforestry As A Means of Alleviating Poverty in Sri LankaArjuna SeneviratneBelum ada peringkat
- FleaDokumen23 halamanFleaAAREEZ IMRAANBelum ada peringkat
- Cations and Anions in Fresh Fruit Juice by Fast Ion ChromatographyDokumen8 halamanCations and Anions in Fresh Fruit Juice by Fast Ion ChromatographyAravinthBelum ada peringkat
- Adenium PropogationDokumen1 halamanAdenium PropogationTanBelum ada peringkat
- Life Processes Class 10 Notes BiologyDokumen8 halamanLife Processes Class 10 Notes BiologyEashurock KnigamBelum ada peringkat