Anda mungkin juga menyukai
- Thyroid Disorders: Tapan A. Patel Cuong Nguyen Mona JamaldinianDokumen41 halamanThyroid Disorders: Tapan A. Patel Cuong Nguyen Mona Jamaldiniansheila_kohBelum ada peringkat
- Hepatotoxicity, Vasculitis:: Pruritic Rash, Arthralgias-Joint Pain, AgranulocytosisDokumen3 halamanHepatotoxicity, Vasculitis:: Pruritic Rash, Arthralgias-Joint Pain, AgranulocytosisThuan Tăng NguyenBelum ada peringkat
- Endocrinology Board Review: Thyroid DisordersDokumen46 halamanEndocrinology Board Review: Thyroid DisordersDemuel Dee L. BertoBelum ada peringkat
- Kuliah HyperthyroidDokumen18 halamanKuliah HyperthyroidFreddyBelum ada peringkat
- Thyroid Gland Diseases in ChildrenDokumen29 halamanThyroid Gland Diseases in ChildrenadinayBelum ada peringkat
- 27 - CC SAN ANTONIO - Hypothyroidism, Hyper, Thyroid Nodular Disease and CancerDokumen77 halaman27 - CC SAN ANTONIO - Hypothyroidism, Hyper, Thyroid Nodular Disease and CancerDann San AntonioBelum ada peringkat
- Antithyroid Drugs: Dr. Novita Carolia, M.Sc. Pharmacology and Therapy Faculty of Medicine Lampung UniversityDokumen26 halamanAntithyroid Drugs: Dr. Novita Carolia, M.Sc. Pharmacology and Therapy Faculty of Medicine Lampung Universitynovita caroliaBelum ada peringkat
- Antithyroid Drugs: Dr. Novita Carolia, M.Sc. Pharmacology and Therapy Faculty of Medicine Lampung UniversityDokumen26 halamanAntithyroid Drugs: Dr. Novita Carolia, M.Sc. Pharmacology and Therapy Faculty of Medicine Lampung UniversityDhita Dwi NandaBelum ada peringkat
- Thyroid Gland and Diseases of Thyroid Gland: DR - Ranadhi Das MD - PGT, Dept of PhysiologyDokumen75 halamanThyroid Gland and Diseases of Thyroid Gland: DR - Ranadhi Das MD - PGT, Dept of Physiologysam mehraBelum ada peringkat
- Clinical Approach of Thyroid Disorders: Hypothyroidsm and HyperthyroidsmDokumen73 halamanClinical Approach of Thyroid Disorders: Hypothyroidsm and HyperthyroidsmdiniBelum ada peringkat
- Pharmacotherapy - Thyroid Disorder PDFDokumen63 halamanPharmacotherapy - Thyroid Disorder PDFnadiah100% (3)
- PBL 1 ThyrotoxicosisDokumen7 halamanPBL 1 ThyrotoxicosishappyhappylandBelum ada peringkat
- Thyrotoxicosis & Hypothyroidism by Prof DR NK ChopraDokumen52 halamanThyrotoxicosis & Hypothyroidism by Prof DR NK ChopraAbdulsalam DostBelum ada peringkat
- Hyperthyroid DisordersDokumen49 halamanHyperthyroid Disordersayu permata dewiBelum ada peringkat
- Thyroid Disorders Chapter 20 Hal 176 Dipiro Edisi 9Dokumen7 halamanThyroid Disorders Chapter 20 Hal 176 Dipiro Edisi 9Nila LutfiBelum ada peringkat
- 2 TSHDokumen7 halaman2 TSHNashat SaadiBelum ada peringkat
- Thyroid & Anti-Thyroid DrugsDokumen59 halamanThyroid & Anti-Thyroid DrugsNiranjanBelum ada peringkat
- Thyroid DisorderDokumen60 halamanThyroid DisorderThe AbyssinicansBelum ada peringkat
- Thyroid DisorderDokumen10 halamanThyroid DisorderDr-Mohammed ElsawyBelum ada peringkat
- Lect 5Dokumen26 halamanLect 5eslambasuony98Belum ada peringkat
- Antithyroid Drugs: Pharmacology and Therapy Faculty of Medicine Lampung UniversityDokumen26 halamanAntithyroid Drugs: Pharmacology and Therapy Faculty of Medicine Lampung UniversityRiska PriyaniBelum ada peringkat
- Morning ReportDokumen31 halamanMorning Reports1882Belum ada peringkat
- Theme 2: Thyroid Diseases: Study GoalsDokumen9 halamanTheme 2: Thyroid Diseases: Study GoalsOlesyaBelum ada peringkat
- Gangguan TiroidDokumen37 halamanGangguan Tiroidjung hoseokBelum ada peringkat
- F1) P-Thyroid DisordersDokumen9 halamanF1) P-Thyroid Disordersstella.gillesania.chenBelum ada peringkat
- Internal Med. EndoDokumen35 halamanInternal Med. EndoEdwin OkonBelum ada peringkat
- Thyrotoxicosis: Presenter: Emiacu Kenneth Facilitator: Dr. Freddie KibengoDokumen35 halamanThyrotoxicosis: Presenter: Emiacu Kenneth Facilitator: Dr. Freddie KibengoNinaBelum ada peringkat
- Thyroid Gland L-Thyroxine (T4) Vs Triiodothyronine (T3) : Follicular CellsDokumen7 halamanThyroid Gland L-Thyroxine (T4) Vs Triiodothyronine (T3) : Follicular CellsPrincess Noreen SavellanoBelum ada peringkat
- Thyroid Disorders - 2023Dokumen82 halamanThyroid Disorders - 2023JEPHTHAH KWASI DANSOBelum ada peringkat
- 3 ThyroidDokumen60 halaman3 ThyroidyeabsraBelum ada peringkat
- Hyperthyroidsm: EpidemiologyDokumen6 halamanHyperthyroidsm: EpidemiologyEllieBelum ada peringkat
- Thyroid Disorders: DR Raghuveer ChoudharyDokumen53 halamanThyroid Disorders: DR Raghuveer ChoudharyPhysiology by Dr RaghuveerBelum ada peringkat
- Thyroid DisordersDokumen34 halamanThyroid DisordersAbdulhameed Mohamed100% (1)
- Hypothyroid in Pregnancy Andi CakraDokumen32 halamanHypothyroid in Pregnancy Andi CakraCakraEkkyBelum ada peringkat
- Congenital Hypothyroidism by ManaDokumen20 halamanCongenital Hypothyroidism by Manamanabhanjanmund420Belum ada peringkat
- Medical and Surgical Complications in Pregnancy: Ramon M. Gonzalez, MDDokumen161 halamanMedical and Surgical Complications in Pregnancy: Ramon M. Gonzalez, MDaldeeray01Belum ada peringkat
- Hyperthyroidism .... 2Dokumen13 halamanHyperthyroidism .... 2guptaavni0000Belum ada peringkat
- Pharmacotherapy Thyroid Disorder UKAIDokumen52 halamanPharmacotherapy Thyroid Disorder UKAIHASNA NURFITRIYATIBelum ada peringkat
- Hyperthyroidism and HypothyroidismDokumen59 halamanHyperthyroidism and HypothyroidismJun AmaroBelum ada peringkat
- Diagnosis and Management of Hyperthyroidism, A Rational ApproachDokumen35 halamanDiagnosis and Management of Hyperthyroidism, A Rational ApproachANCHAL SHARMABelum ada peringkat
- Thyroid Gland An Diseases of Thyroid D Gland: Omc LectureDokumen59 halamanThyroid Gland An Diseases of Thyroid D Gland: Omc LectureEdward MakemboBelum ada peringkat
- Thyrotoxicosi S: Dr.P.Viswakumar M.S Assistant Professor, Dept of General Surgery, PsgimsrDokumen57 halamanThyrotoxicosi S: Dr.P.Viswakumar M.S Assistant Professor, Dept of General Surgery, PsgimsrpurnaBelum ada peringkat
- Thyroid DiseasesDokumen65 halamanThyroid DiseasesSahirBelum ada peringkat
- Pathophysiology and Principles of TreatmentDokumen1 halamanPathophysiology and Principles of TreatmentreavaldyakamichiBelum ada peringkat
- Thyroid DisordersDokumen55 halamanThyroid DisordersNsubuga Ivan100% (1)
- Pharmacology AssignmentDokumen6 halamanPharmacology AssignmentMaria MushtaqueBelum ada peringkat
- Management and Medications in Thyroid Strom and Myxoedema ComaDokumen41 halamanManagement and Medications in Thyroid Strom and Myxoedema ComaBhavesh kunvarBelum ada peringkat
- Therapeutics: Thyroid DisordersDokumen24 halamanTherapeutics: Thyroid DisordersSharas FarhadBelum ada peringkat
- Week 3 Pharmaco Part 2Dokumen34 halamanWeek 3 Pharmaco Part 2Tiko JomidavaBelum ada peringkat
- ThyrotoxicosisDokumen105 halamanThyrotoxicosisAli Murtaza Abbas100% (1)
- 02 Lecture 10 Anti-Thyroid Drugs (DR Thatcher Pod Pharm 2022)Dokumen36 halaman02 Lecture 10 Anti-Thyroid Drugs (DR Thatcher Pod Pharm 2022)sahilaminBelum ada peringkat
- Hyperthyoidism: Anaesthetic ManagementDokumen11 halamanHyperthyoidism: Anaesthetic ManagementerzaraptorBelum ada peringkat
- HyperthyroidismDokumen3 halamanHyperthyroidismNUR 'ALIA SUFIA BINTI AMRANBelum ada peringkat
- LO&WO - Endokrin.week4 (Michael G)Dokumen6 halamanLO&WO - Endokrin.week4 (Michael G)Michael GBelum ada peringkat
- Anti-Thyroid and Thyroid DrugsDokumen36 halamanAnti-Thyroid and Thyroid DrugsDylan MansillaBelum ada peringkat
- Hperthyroidism 1Dokumen4 halamanHperthyroidism 1Salwa KaramanBelum ada peringkat
- Thyroid and ParathyroidDokumen29 halamanThyroid and Parathyroidpranutan739Belum ada peringkat
- THYROID Disorders For PB BSCDokumen81 halamanTHYROID Disorders For PB BSCchetankumarbhumireddy50% (2)
- DR - Dai-Thyroid Antithyroid DrugsDokumen37 halamanDR - Dai-Thyroid Antithyroid DrugsNguyễn Tấn TàiBelum ada peringkat
- Thyroid Diet: How to improve and cure thyroid disorders, lose weight, and improve metabolism with the help of food!Dari EverandThyroid Diet: How to improve and cure thyroid disorders, lose weight, and improve metabolism with the help of food!Belum ada peringkat
- Brightstar 2317 EnglDokumen1 halamanBrightstar 2317 EnglNavin ChandrasekaranBelum ada peringkat
- 600% in 6 Days: How To Make Fantastic Returns On Your Money at The Casino Playing RouletteDokumen19 halaman600% in 6 Days: How To Make Fantastic Returns On Your Money at The Casino Playing RouletteNavin ChandrasekaranBelum ada peringkat
- Leeden Safety Catalogue 2010 - Personal ProtectionDokumen44 halamanLeeden Safety Catalogue 2010 - Personal ProtectionNavin ChandrasekaranBelum ada peringkat
- How To Raise A Smart KidDokumen9 halamanHow To Raise A Smart KidNavin ChandrasekaranBelum ada peringkat
- Sri Siva - MantrasDokumen119 halamanSri Siva - Mantrasharryhowser100% (24)
- A Practical Guide To Technical Indicators Moving AveragesDokumen9 halamanA Practical Guide To Technical Indicators Moving Averagesfarangeston100% (4)
- 6th Central Pay Commission Salary CalculatorDokumen15 halaman6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- Chapter 2 - Output DevicesDokumen32 halamanChapter 2 - Output DevicesNavin ChandrasekaranBelum ada peringkat
- Michael Saso Tantric Art and MeditationDokumen114 halamanMichael Saso Tantric Art and Meditationsinisa937056100% (5)
- Cardiac Output: Cardiac Output Heart Rate X Stroke Volume CO HR X SVDokumen4 halamanCardiac Output: Cardiac Output Heart Rate X Stroke Volume CO HR X SVNavin ChandrasekaranBelum ada peringkat
- Higher Education Updates 25Dokumen33 halamanHigher Education Updates 25Navin ChandrasekaranBelum ada peringkat
- Chapter 5 - Communication & NetworkDokumen42 halamanChapter 5 - Communication & NetworkNavin ChandrasekaranBelum ada peringkat
- A Glass of MilkDokumen20 halamanA Glass of Milksupaporn-nilayakanonBelum ada peringkat
- PPS With Sound. Click For Next ImageDokumen17 halamanPPS With Sound. Click For Next ImageNavin ChandrasekaranBelum ada peringkat
- Chapter 7 - E - CommerceDokumen19 halamanChapter 7 - E - CommerceNavin ChandrasekaranBelum ada peringkat
- Om Kleem Krishnaye Shreem Brzee Lakshmiye Sameda Guru Dattatreya Siva Baba SwahaaaaDokumen1 halamanOm Kleem Krishnaye Shreem Brzee Lakshmiye Sameda Guru Dattatreya Siva Baba SwahaaaaNavin ChandrasekaranBelum ada peringkat
- Om Kleem Krishnaye Shreem Brzee Lakshmiye Sameda Guru Dattatreya Siva Baba SwahaaaaDokumen1 halamanOm Kleem Krishnaye Shreem Brzee Lakshmiye Sameda Guru Dattatreya Siva Baba SwahaaaaNavin ChandrasekaranBelum ada peringkat
- Air Worksheet For Tour/Package: Date Agent Name I.D. Number To The Attention ofDokumen1 halamanAir Worksheet For Tour/Package: Date Agent Name I.D. Number To The Attention ofNavin ChandrasekaranBelum ada peringkat
- Batik ProcessDokumen2 halamanBatik ProcessNavin ChandrasekaranBelum ada peringkat
- TM® Mantras, Techniques, and Related MethodsDokumen63 halamanTM® Mantras, Techniques, and Related Methodscogumelohead93% (15)
- Challenging HR & IR EnvironmentDokumen61 halamanChallenging HR & IR EnvironmentNavin ChandrasekaranBelum ada peringkat
- A Tantra Nada Kriya ALL Picture TextDokumen121 halamanA Tantra Nada Kriya ALL Picture Textjasnajoga0% (1)
- Workplace Dispute ResolutionDokumen55 halamanWorkplace Dispute ResolutionNavin ChandrasekaranBelum ada peringkat
- Shakti Suu TraDokumen3 halamanShakti Suu TraNavin ChandrasekaranBelum ada peringkat
- Adi NathaDokumen12 halamanAdi NathaNavin Chandrasekaran100% (3)
- Svatantram Te Tantram Khsiti Talam AvatitaradidamDokumen1 halamanSvatantram Te Tantram Khsiti Talam AvatitaradidamNavin ChandrasekaranBelum ada peringkat
- Magic of KaliDokumen0 halamanMagic of KaliBala MBelum ada peringkat
- YoginiDokumen14 halamanYoginiNavin ChandrasekaranBelum ada peringkat
- Chinna MaDokumen2 halamanChinna MaNavin ChandrasekaranBelum ada peringkat
- Chapter 22: The Thyroid Gland: by Marissa Grotzke, Dev AbrahamDokumen21 halamanChapter 22: The Thyroid Gland: by Marissa Grotzke, Dev AbrahamJanielle FajardoBelum ada peringkat
- 30 - Toronto Notes 2011 - Common Unit Conversions - Commonly Measured Laboratory Values - Abbreviations - IndexDokumen28 halaman30 - Toronto Notes 2011 - Common Unit Conversions - Commonly Measured Laboratory Values - Abbreviations - IndexRazrin RazakBelum ada peringkat
- Anatomy Endocrine Q and ADokumen16 halamanAnatomy Endocrine Q and ASamantha Frey LopezBelum ada peringkat
- Endocrine MedicationsDokumen47 halamanEndocrine MedicationsAamir AzizBelum ada peringkat
- Hipo - Hiper SubDokumen123 halamanHipo - Hiper SubdankouzielBelum ada peringkat
- Thyroid 2Dokumen16 halamanThyroid 2Haneef SafvanBelum ada peringkat
- Sem 4 MCQ Week 4 Jan 2014 CTL McqsDokumen15 halamanSem 4 MCQ Week 4 Jan 2014 CTL McqsFlowerBelum ada peringkat
- British Homeopathic AssociationDokumen195 halamanBritish Homeopathic AssociationNasarMahmoodBelum ada peringkat
- Isfm HipertiroidismoDokumen17 halamanIsfm HipertiroidismoMaria Rodriguez RodrguezBelum ada peringkat
- 1 SpecForce Abs Manual For MenDokumen115 halaman1 SpecForce Abs Manual For MenGilberto Solares100% (2)
- GugulipidDokumen7 halamanGugulipidManish WadhwaniBelum ada peringkat
- Iodine and Iron DeficienciesDokumen145 halamanIodine and Iron DeficienciesAtika SugiartoBelum ada peringkat
- K13-14 - Fisiologi Hormon Tiroid, Paratiroid, Dan AdrenalDokumen62 halamanK13-14 - Fisiologi Hormon Tiroid, Paratiroid, Dan AdrenalMuhammad Ikhram Habib DaulayBelum ada peringkat
- Clinical Practice Guidelines For The Management of HypothyroidismDokumen41 halamanClinical Practice Guidelines For The Management of HypothyroidismShannya PuaBelum ada peringkat
- ENDOCRINE DISORDERS (Autosaved)Dokumen81 halamanENDOCRINE DISORDERS (Autosaved)Princewill SeiyefaBelum ada peringkat
- Thyroid DiseaseDokumen30 halamanThyroid Diseasemy Lord JesusBelum ada peringkat
- CLIA Acceptable Test Performance CriteriaDokumen4 halamanCLIA Acceptable Test Performance CriteriaMihaelaHorgaBelum ada peringkat
- Pathophysiology of DepressionDokumen44 halamanPathophysiology of DepressionArmando Marín FloresBelum ada peringkat
- Chemical Coordination and ControlDokumen18 halamanChemical Coordination and ControlGovind RajputBelum ada peringkat
- Tutorial On Goiter GadedDokumen117 halamanTutorial On Goiter GadedhindabdalgadirBelum ada peringkat
- 14 - Interferences in Immunoassay PDFDokumen16 halaman14 - Interferences in Immunoassay PDFLyannYisellBelum ada peringkat
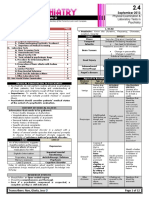
- 02.04. Physical Examination and Laboratory Tests in PsychiatryDokumen12 halaman02.04. Physical Examination and Laboratory Tests in PsychiatryMiguel C. DolotBelum ada peringkat
- Thyroid Disorders: Hyperthyroidism HypothyroidismDokumen66 halamanThyroid Disorders: Hyperthyroidism HypothyroidismGabz GabbyBelum ada peringkat
- Synevo Results 3001981811Dokumen3 halamanSynevo Results 3001981811Edward MarinescuBelum ada peringkat
- Memon Medical Institute Hospital: Laboratory Rate ListDokumen26 halamanMemon Medical Institute Hospital: Laboratory Rate List1123456789000% (1)
- Anesthesia For Pituitary Lesions: Rialph Engel D. GuiaDokumen57 halamanAnesthesia For Pituitary Lesions: Rialph Engel D. GuiaDoc SabBelum ada peringkat
- Thyroid Hormones & Anti Thyroid AgentsDokumen3 halamanThyroid Hormones & Anti Thyroid AgentsJaybee SarmientoBelum ada peringkat
- Alprazolam Effect On ThyroidDokumen7 halamanAlprazolam Effect On ThyroidswatiBelum ada peringkat
- TDAH ADHD e Def de Iodo 2004Dokumen7 halamanTDAH ADHD e Def de Iodo 2004Pollyana Furtado JunqueiraBelum ada peringkat
- Drugs Affecting The Endocrine System - PharmacologyDokumen58 halamanDrugs Affecting The Endocrine System - PharmacologyMuhammad Riandy Lukman TanjungBelum ada peringkat