Anda mungkin juga menyukai
- 07 PtosisDokumen25 halaman07 PtosisAndriani Kemala SariBelum ada peringkat
- Classification of Ptosis: 1. NeurogenicDokumen25 halamanClassification of Ptosis: 1. NeurogenicMuliany PratiwiBelum ada peringkat
- MeningiomaDokumen51 halamanMeningiomaarushijha2000Belum ada peringkat
- Neurology Equations Made Simple: Differential Diagnosis and NeuroemergenciesDari EverandNeurology Equations Made Simple: Differential Diagnosis and NeuroemergenciesBelum ada peringkat
- Optic NeuritisDokumen31 halamanOptic NeuritisUsman ImtiazBelum ada peringkat
- Eyelids Diseases Lacrimal System DiseasesDokumen45 halamanEyelids Diseases Lacrimal System DiseasesMAMA LALABelum ada peringkat
- Thyroid Eye Disease: DR Aleena ShahDokumen33 halamanThyroid Eye Disease: DR Aleena ShahhamsBelum ada peringkat
- Double Vision / Diplopia: Dr. R. Handoko Pratomo, SPMDokumen94 halamanDouble Vision / Diplopia: Dr. R. Handoko Pratomo, SPMNefri TiawarmanBelum ada peringkat
- 30secondary GlaucomasDokumen15 halaman30secondary GlaucomasShari' Si WahyuBelum ada peringkat
- 30secondary GlaucomasDokumen19 halaman30secondary GlaucomasShari' Si WahyuBelum ada peringkat
- Embryologic DefectsDokumen62 halamanEmbryologic DefectsBenjamin AgbonzeBelum ada peringkat
- Retina Nss2013Dokumen46 halamanRetina Nss2013proluvieslacusBelum ada peringkat
- 7 Peripheral Neuropathy MyopathyDokumen83 halaman7 Peripheral Neuropathy Myopathymuhammadridhwan100% (1)
- Dr. Bhosale SystemicDokumen87 halamanDr. Bhosale SystemicdrksuhasBelum ada peringkat
- Approach To A Case of DiplopiaDokumen63 halamanApproach To A Case of DiplopiaSriniwasBelum ada peringkat
- Thyroid Eye Disease: - Varshaa BDokumen16 halamanThyroid Eye Disease: - Varshaa BRia SharmaBelum ada peringkat
- PAED MicrocephalyDokumen18 halamanPAED Microcephalyaboje ochekwuBelum ada peringkat
- Developmental Disturbances of Oral Cavity-KushDokumen405 halamanDevelopmental Disturbances of Oral Cavity-KushKush PathakBelum ada peringkat
- 1400546814.1633unit 10 Nervous System PathophysiologyDokumen27 halaman1400546814.1633unit 10 Nervous System PathophysiologyRyan Adi PutraBelum ada peringkat
- 6 - Intracranial MassDokumen5 halaman6 - Intracranial MassAmmarBelum ada peringkat
- Eyedocs Excerpts PediatricsDokumen14 halamanEyedocs Excerpts PediatricsMunib ur RehmanBelum ada peringkat
- Thyroid OphthalmopathyDokumen59 halamanThyroid OphthalmopathyLavanya MadabushiBelum ada peringkat
- RADIOLOGI - NEURORADIOLOGI 2 - Dr. Farah - Kelas ADokumen106 halamanRADIOLOGI - NEURORADIOLOGI 2 - Dr. Farah - Kelas ASeno TanubrataBelum ada peringkat
- Slides For Pediatric Osce ExamDokumen389 halamanSlides For Pediatric Osce Examadan yare100% (1)
- Pathology of The CnsDokumen38 halamanPathology of The Cnscy lifeBelum ada peringkat
- Corneal DiseasesDokumen32 halamanCorneal Diseasesnighat khanBelum ada peringkat
- Multiple Sclerosis (Medicalstudyzone - Com)Dokumen21 halamanMultiple Sclerosis (Medicalstudyzone - Com)WaleedBelum ada peringkat
- Grave'S Disease: Dr. Ibrahim, SPMDokumen24 halamanGrave'S Disease: Dr. Ibrahim, SPMAnisa Karamina WardaniBelum ada peringkat
- Paediatric NeurophthalmologyDokumen49 halamanPaediatric NeurophthalmologyNavami KrishnaBelum ada peringkat
- Good MorningDokumen76 halamanGood MorningCSE-A-2022-RAJESWARI NBelum ada peringkat
- Menongioma PPT Slidshare PDFDokumen75 halamanMenongioma PPT Slidshare PDFranggaBelum ada peringkat
- Pupillary DisorderDokumen19 halamanPupillary DisorderWan HafizBelum ada peringkat
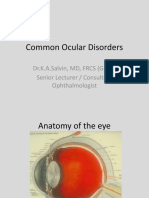
- Common Ocular DisordersDokumen108 halamanCommon Ocular DisordersKa SalvinBelum ada peringkat
- Diseases of Nerves and MusclesDokumen46 halamanDiseases of Nerves and MusclesAME DENTAL COLLEGE RAICHUR, KARNATAKABelum ada peringkat
- Glaucoma and TinnitusDokumen20 halamanGlaucoma and Tinnitusqurat-ul-ain.sonBelum ada peringkat
- Neurocutaneous DisorderDokumen20 halamanNeurocutaneous DisorderBarez AminBelum ada peringkat
- DermatologyDokumen223 halamanDermatologySahan EpitawalaBelum ada peringkat
- Herpes Zoster: Bing-Rong ZHOUDokumen43 halamanHerpes Zoster: Bing-Rong ZHOUMichael Jansen Sulaiman100% (1)
- Brain Tumor and Clinical FindingsDokumen21 halamanBrain Tumor and Clinical FindingsAlbert Ciam100% (1)
- Neurocutaneous SyndromesDokumen91 halamanNeurocutaneous SyndromesShakib ShafiBelum ada peringkat
- MicrophtalmiaDokumen5 halamanMicrophtalmiaMuhammad AdilBelum ada peringkat
- Glaucoma & CataractDokumen53 halamanGlaucoma & CataractBenita100% (1)
- Neuro Ophthalmology PDFDokumen70 halamanNeuro Ophthalmology PDFSurat Tanprawate100% (4)
- Nervous System (S.S)Dokumen112 halamanNervous System (S.S)Suman ShahBelum ada peringkat
- 2019 Dr. Halida 1. Retinopati DiabetikafixDokumen44 halaman2019 Dr. Halida 1. Retinopati DiabetikafixLuthfia WardhaniBelum ada peringkat
- Dermatology: Minci YazuminDokumen48 halamanDermatology: Minci Yazuminminci senseiBelum ada peringkat
- Disease of Lids and Lacrim Al Apparatus: The First Affiliated Hospital of Zhengzhou UniversityDokumen46 halamanDisease of Lids and Lacrim Al Apparatus: The First Affiliated Hospital of Zhengzhou Universityapi-19916399Belum ada peringkat
- Trisomy 21-Down Syndrome: Payal DhakappaDokumen35 halamanTrisomy 21-Down Syndrome: Payal DhakappaPayal AmarnathBelum ada peringkat
- Semiology Lecture 4. Facies, Neck, ThyroidDokumen59 halamanSemiology Lecture 4. Facies, Neck, ThyroidmlinaballerinaBelum ada peringkat
- Complications of SinusitisDokumen42 halamanComplications of SinusitisdrsadafrafiBelum ada peringkat
- Neuritis OpticDokumen13 halamanNeuritis OpticBimo Nugroho saktiBelum ada peringkat
- Retinal Disorders Med VDokumen66 halamanRetinal Disorders Med Vhenok birukBelum ada peringkat
- Facial PalsyDokumen25 halamanFacial PalsyMahad abuukarBelum ada peringkat
- Optic Disc: Symptoms of The Optic Nerve DiseasesDokumen11 halamanOptic Disc: Symptoms of The Optic Nerve DiseasesDilawar JanBelum ada peringkat
- Diseases of Endocrine SystemDokumen84 halamanDiseases of Endocrine SystemDuaa The PandaBelum ada peringkat
- Facial PalsyDokumen33 halamanFacial PalsyArista SBelum ada peringkat
- Overview of Pediatric GeneticsDokumen12 halamanOverview of Pediatric Geneticsnicdeep100% (1)
- Motor Neuron DiseaseDokumen23 halamanMotor Neuron DiseaseNaman MishraBelum ada peringkat
- Ptosis 03presenDokumen26 halamanPtosis 03presentotalrevoltBelum ada peringkat
- AIDS in The Workplace LawDokumen30 halamanAIDS in The Workplace LawPacific SpectrumBelum ada peringkat
- (Robert Sallares) Malaria and Rome A History of MDokumen358 halaman(Robert Sallares) Malaria and Rome A History of Mclaudia lilianaBelum ada peringkat
- Laporan Divisi Nefrologi 3 Maret 2020Dokumen18 halamanLaporan Divisi Nefrologi 3 Maret 2020annisanangBelum ada peringkat
- Pharmacology Fundamental ConceptsDokumen84 halamanPharmacology Fundamental Conceptsteaforschool filesBelum ada peringkat
- Cicatrización ImplanteDokumen18 halamanCicatrización Implantejorge sepulvedaBelum ada peringkat
- DRISHTIDokumen1 halamanDRISHTIsumitha SBelum ada peringkat
- English - Modern vs. Traditional MedicineDokumen11 halamanEnglish - Modern vs. Traditional MedicineJoao AlfandegaBelum ada peringkat
- Alprazolam Effect On ThyroidDokumen7 halamanAlprazolam Effect On ThyroidswatiBelum ada peringkat
- Answer and Rationale Community Health NursingDokumen25 halamanAnswer and Rationale Community Health NursingDENNIS N. MUÑOZ100% (1)
- Salivary Glands For BDSDokumen47 halamanSalivary Glands For BDSSnighdayBelum ada peringkat
- Patient Practitioner Remedy PDFDokumen9 halamanPatient Practitioner Remedy PDFAugustusBelum ada peringkat
- Daftar Obat Kapal REKOMENDASI WHO 3RD Rev KKP SemarangDokumen1 halamanDaftar Obat Kapal REKOMENDASI WHO 3RD Rev KKP Semaranganon_914901469Belum ada peringkat
- Bronchial AsthmaDokumen40 halamanBronchial Asthmasamson bd mokuntil100% (1)
- Neuroshield ReportDokumen2 halamanNeuroshield Reportrahim pathanBelum ada peringkat
- WNHS Og AntepartumHaemorrhageDokumen17 halamanWNHS Og AntepartumHaemorrhagelydia amaliaBelum ada peringkat
- Mri Report - Left Knee Joint: Name Patient ID Accession No Age/Gender Referred by DateDokumen2 halamanMri Report - Left Knee Joint: Name Patient ID Accession No Age/Gender Referred by Datefaiyaz432Belum ada peringkat
- CerebrolysinDokumen1 halamanCerebrolysineiad-mahmoudBelum ada peringkat
- Duchenne Muscular DystrophyDokumen9 halamanDuchenne Muscular Dystrophyapi-306057885Belum ada peringkat
- Pulmonary and Critical Care MedicineDokumen48 halamanPulmonary and Critical Care MedicineCarlos HernándezBelum ada peringkat
- Laporan Obat Sesuai Formularium Maret 2019Dokumen22 halamanLaporan Obat Sesuai Formularium Maret 2019Maria AmabiBelum ada peringkat
- Research ProposalDokumen25 halamanResearch ProposaladerindBelum ada peringkat
- Trace Element and Oral Health PedoDokumen49 halamanTrace Element and Oral Health PedoFourthMolar.com100% (1)
- Arthritis Protocol 1Dokumen11 halamanArthritis Protocol 1Co Bay-AgiBelum ada peringkat
- WC500059147 PDFDokumen140 halamanWC500059147 PDFAnaStankovićBelum ada peringkat
- 5z23. ED Crowding Overview and Toolkit (Dec 2015)Dokumen33 halaman5z23. ED Crowding Overview and Toolkit (Dec 2015)Peter 'Pierre' RobsonBelum ada peringkat
- Case Study For Beta Acute Lymphoblastic Leukemia (B-All)Dokumen15 halamanCase Study For Beta Acute Lymphoblastic Leukemia (B-All)Shakira HashimBelum ada peringkat
- Conization of CervixDokumen4 halamanConization of Cervixdrnareshkumar3281Belum ada peringkat
- Grade 4 Chondromalacia Patella TreatmentDokumen3 halamanGrade 4 Chondromalacia Patella TreatmentTroy0% (1)
- BC CancerDokumen42 halamanBC CancerIsal SparrowBelum ada peringkat
- Kankushta (One of The Uparasas in Rasashastra)Dokumen13 halamanKankushta (One of The Uparasas in Rasashastra)Ayurveda PPT0% (1)