Anda mungkin juga menyukai
- Guildelines For Hiv Testing NacoDokumen165 halamanGuildelines For Hiv Testing NacoNagendra Singh BeniwalBelum ada peringkat
- Journal Reading THT OEDokumen22 halamanJournal Reading THT OEFahmy Zaeni DahlanBelum ada peringkat
- Efektivitas Antibiotik Pada Kaki DiabetikDokumen6 halamanEfektivitas Antibiotik Pada Kaki DiabetikFawzia Haznah Nurul ImaniBelum ada peringkat
- Referat OsteomielitisDokumen22 halamanReferat OsteomielitisDexel Putra Simbolon100% (1)
- CamScanner Document ScansDokumen68 halamanCamScanner Document Scanspramuliansyah haqBelum ada peringkat
- MK Giz Slide Malnutrisi Energi ProteinDokumen88 halamanMK Giz Slide Malnutrisi Energi ProteinAri AndryBelum ada peringkat
- Eritro Papulo Skuamosa 2021Dokumen47 halamanEritro Papulo Skuamosa 2021Yolanda Agnesia Purba0% (1)
- Tatalaksana Pada Luka BakarDokumen55 halamanTatalaksana Pada Luka Bakarmagdalena sriBelum ada peringkat
- HEMOROIDDokumen29 halamanHEMOROIDDanang Aryo PinujiBelum ada peringkat
- Dr. Jufri Latief (Compartment Syndromes)Dokumen11 halamanDr. Jufri Latief (Compartment Syndromes)shintaBelum ada peringkat
- Referat Kandidosis Kutis - Dhira Dan A. Fari-70700120034 Dan 038Dokumen14 halamanReferat Kandidosis Kutis - Dhira Dan A. Fari-70700120034 Dan 038Ahmad Fari Arief LopaBelum ada peringkat
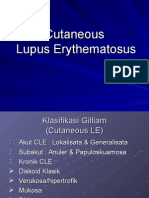
- Cutaneous Lupus ErythematosusDokumen15 halamanCutaneous Lupus ErythematosusErika KusumawatiBelum ada peringkat
- Anatomi, Eflouresensi KulitDokumen67 halamanAnatomi, Eflouresensi KulitWhydia Wedha SutedjaBelum ada peringkat
- Journal ReadingDokumen18 halamanJournal ReadingnafisyarifahBelum ada peringkat
- Vitamin D Levels and Recurrent Tonsillitis in ChildrenDokumen14 halamanVitamin D Levels and Recurrent Tonsillitis in ChildrenMyarBelum ada peringkat
- Diabetic Foot Ulcer ClassificationDokumen17 halamanDiabetic Foot Ulcer ClassificationAriski Pratama JohanBelum ada peringkat
- Referat Kulit KakayDokumen26 halamanReferat Kulit KakayRezky Dwiputra FellanysBelum ada peringkat
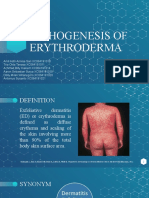
- Group 5 - Pathogenesis of ErythrodermaDokumen20 halamanGroup 5 - Pathogenesis of Erythrodermaachmad billy hakiemBelum ada peringkat
- CLARA SKIN Who PDFDokumen154 halamanCLARA SKIN Who PDFhasnul ramadhaniBelum ada peringkat
- Gnaps EmedicineDokumen13 halamanGnaps Emedicineharyanti lupitaBelum ada peringkat
- Spondilitis TB AnakDokumen36 halamanSpondilitis TB Anaktry intan kartini50% (2)
- Vaginosis BakterialisDokumen9 halamanVaginosis BakterialisIntan PermataBelum ada peringkat
- Jurnal AcneDokumen5 halamanJurnal AcneStacy VaniaBelum ada peringkat
- Frakture of SpineDokumen26 halamanFrakture of SpinePaskah MianBelum ada peringkat
- Guyon's Canal SyndromeDokumen7 halamanGuyon's Canal SyndromeBakhrul IlmeeBelum ada peringkat
- Dr. I DEWA PUTU SP - PD KGer - TATALAKSANA FARMAKOLOGIK TERBARU HIPERURISEMIA DAN GOUT USIA LANJUTDokumen51 halamanDr. I DEWA PUTU SP - PD KGer - TATALAKSANA FARMAKOLOGIK TERBARU HIPERURISEMIA DAN GOUT USIA LANJUTCOVID RSHJBelum ada peringkat
- Dermatological Infection Management UpdateDokumen29 halamanDermatological Infection Management UpdateyheyenBelum ada peringkat
- Abdominal Lump-Nurcahyo Setiawan (2016) - 2Dokumen95 halamanAbdominal Lump-Nurcahyo Setiawan (2016) - 2RobertOktaChandraBelum ada peringkat
- Referat Osteogenesis ImperfectaDokumen21 halamanReferat Osteogenesis ImperfectaArdhian RamadhanBelum ada peringkat
- Liver Cancer Staging and Treatment OptionsDokumen37 halamanLiver Cancer Staging and Treatment OptionsSyifa FadyaBelum ada peringkat
- LimfadenopatiDokumen8 halamanLimfadenopatiZulkarnain PrakosoBelum ada peringkat
- Disseminated Intravacular Coagulation (DIC) 2Dokumen12 halamanDisseminated Intravacular Coagulation (DIC) 2Radya AgnaBelum ada peringkat
- FFS Jambaf Aug2021Dokumen2 halamanFFS Jambaf Aug2021royescspchiitymmuaBelum ada peringkat
- Olanzapine Vs AripiprazoleDokumen8 halamanOlanzapine Vs AripiprazoleDivaviyaBelum ada peringkat
- Drug Eruption Fix PrintDokumen30 halamanDrug Eruption Fix PrintAshari MohpulBelum ada peringkat
- Dr. Ago Harlim - MikosisDokumen50 halamanDr. Ago Harlim - MikosisBrian Pasa NababanBelum ada peringkat
- Eau 2020 - Urological TraumaDokumen47 halamanEau 2020 - Urological TraumaDidy KurniawanBelum ada peringkat
- 5W FeverDokumen14 halaman5W FeverYork GarcíaBelum ada peringkat
- Sindroma DispepsiaDokumen6 halamanSindroma DispepsiaMifta Paramitha MuchlisBelum ada peringkat
- 13 - 266fourniers Gangrene PDFDokumen5 halaman13 - 266fourniers Gangrene PDFMochamad RizalBelum ada peringkat
- Medulla Compression AcuteDokumen46 halamanMedulla Compression AcuteamiraBelum ada peringkat
- Akut SkrotumDokumen26 halamanAkut SkrotumToni PinemBelum ada peringkat
- K23 - Text Book Reading MiopatiDokumen28 halamanK23 - Text Book Reading MiopatiNaila SyifaBelum ada peringkat
- Sexually Transmitted DiseasesDokumen70 halamanSexually Transmitted DiseasesErly MekarsariBelum ada peringkat
- Review Article Bombax Ceiba Linn. Pharma PDFDokumen8 halamanReview Article Bombax Ceiba Linn. Pharma PDFpankaj chaudharyBelum ada peringkat
- Referat PPHDokumen35 halamanReferat PPHSamdiSutantoBelum ada peringkat
- Emergency management of chemical burnsDokumen3 halamanEmergency management of chemical burnsdeasyarizaniBelum ada peringkat
- Rin - O24: Cervicitis Gonorhoea (Vietnam Rose) # Nona AsimptomatikDokumen6 halamanRin - O24: Cervicitis Gonorhoea (Vietnam Rose) # Nona AsimptomatikNurrahma Putrie HapsariBelum ada peringkat
- Anatomi Fisiologi KorneaDokumen11 halamanAnatomi Fisiologi KorneaMauVeeBelum ada peringkat
- Dry EyeDokumen22 halamanDry EyeSilva Neta Oktari100% (1)
- Clinical Science Section: Polip ServiksDokumen15 halamanClinical Science Section: Polip ServiksnsrinanaBelum ada peringkat
- Batu PielumDokumen19 halamanBatu PielumVera OktapianiBelum ada peringkat
- Tutorial Kasus: AppendisitisDokumen50 halamanTutorial Kasus: Appendisitiseruza hiwatariBelum ada peringkat
- Neoplasma MataDokumen65 halamanNeoplasma MataFadilah NSBelum ada peringkat
- Laporan Kasus Skizofrenia ParanoidDokumen63 halamanLaporan Kasus Skizofrenia ParanoidMichi Mich100% (1)
- Palmoplantar PustulosisDokumen3 halamanPalmoplantar PustulosisRobby ZayendraBelum ada peringkat
- Rectal Prolapse PDFDokumen92 halamanRectal Prolapse PDFadel santos100% (2)
- Anorectal MalformationDokumen40 halamanAnorectal Malformationblessy83% (18)
- Imperforate AnusDokumen52 halamanImperforate Anushayssam rashwan100% (6)
- Anorectal MalformationDokumen40 halamanAnorectal MalformationFrankBelum ada peringkat
- ITunes DiagnosticsDokumen2 halamanITunes DiagnosticsIrfandy Chairi Sulaiman LubisBelum ada peringkat
- Practice ECGStripsDokumen300 halamanPractice ECGStripspupuliciouz0% (1)
- Meet ScanbotDokumen4 halamanMeet ScanbotIrfandy Chairi Sulaiman LubisBelum ada peringkat
- JNC 8 Guideline Algorithm for Treating HypertensionDokumen2 halamanJNC 8 Guideline Algorithm for Treating HypertensionTaradifaNurInsi0% (1)
- Ads Applicationform 2014Dokumen30 halamanAds Applicationform 2014Irfandy Chairi Sulaiman LubisBelum ada peringkat
- Sinonasal ReviewDokumen18 halamanSinonasal ReviewZsa Zsa MarananiBelum ada peringkat
- Quick Management Guide in Emergency Medicine v1.0.25 20111208 (Build13)Dokumen156 halamanQuick Management Guide in Emergency Medicine v1.0.25 20111208 (Build13)Anselm Su100% (14)
- Final StepDokumen1 halamanFinal StepIrfandy Chairi Sulaiman LubisBelum ada peringkat
- !!!!!!!!!!!!!!!!!!! First Read This !!!!!!!!!!!!!!!!!!!!!!!Dokumen1 halaman!!!!!!!!!!!!!!!!!!! First Read This !!!!!!!!!!!!!!!!!!!!!!!Irfandy Chairi Sulaiman LubisBelum ada peringkat
- Acute Myocardial Infarction Post CABGDokumen30 halamanAcute Myocardial Infarction Post CABGIrfandy Chairi Sulaiman LubisBelum ada peringkat
- ReadmeDokumen11 halamanReadmeIYogasukma WijayaBelum ada peringkat
- Guidelines NSTE ACSDokumen56 halamanGuidelines NSTE ACSPedro Perez FuentesBelum ada peringkat
- CMD Ni BroDokumen1 halamanCMD Ni BroIrfandy Chairi Sulaiman LubisBelum ada peringkat
- Retail Key Win 8.1Dokumen1 halamanRetail Key Win 8.1Irfandy Chairi Sulaiman LubisBelum ada peringkat
- Atherosclerosis & Trombosis Dr. FaturochmanDokumen50 halamanAtherosclerosis & Trombosis Dr. FaturochmanPutry RizqiaBelum ada peringkat
- Atherosclerosis ACSDokumen38 halamanAtherosclerosis ACSIrfandy Chairi Sulaiman LubisBelum ada peringkat
- Ads Applicationform 2014Dokumen30 halamanAds Applicationform 2014Irfandy Chairi Sulaiman LubisBelum ada peringkat
- Hypertensive Disorders in PregnancyDokumen40 halamanHypertensive Disorders in PregnancyIrfandy Chairi Sulaiman LubisBelum ada peringkat
- St Mary's Adult Blood Transfusion Policy Medical StaffDokumen15 halamanSt Mary's Adult Blood Transfusion Policy Medical StaffStanislaus JosephBelum ada peringkat
- Follow Up HarianDokumen5 halamanFollow Up HarianFikri AnandaBelum ada peringkat
- Anti HistaminDokumen9 halamanAnti HistaminIrfandy Chairi Sulaiman LubisBelum ada peringkat
- Guidelines NSTE ACSDokumen56 halamanGuidelines NSTE ACSPedro Perez FuentesBelum ada peringkat
- Guidelines STEMI EscDokumen38 halamanGuidelines STEMI EscIrfandy Chairi Sulaiman LubisBelum ada peringkat
- Cardiac Failure: by Dr. Osman BukhariDokumen48 halamanCardiac Failure: by Dr. Osman BukhariIrfandy Chairi Sulaiman LubisBelum ada peringkat
- ECG Praktis ParamedikDokumen49 halamanECG Praktis ParamedikIrfandy Chairi Sulaiman LubisBelum ada peringkat
- Asthma Lecture 200705Dokumen77 halamanAsthma Lecture 200705Irfandy Chairi Sulaiman LubisBelum ada peringkat
- Pediatric TB Management Training Diagnosis (Part 2Dokumen56 halamanPediatric TB Management Training Diagnosis (Part 2Irfandy Chairi Sulaiman LubisBelum ada peringkat
- Department of Child Health Faculty of Medicine University of Syiah KualaDokumen55 halamanDepartment of Child Health Faculty of Medicine University of Syiah KualaIrfandy Chairi Sulaiman LubisBelum ada peringkat
- A Pain Education ProgrammeDokumen13 halamanA Pain Education Programmeapi-244230664Belum ada peringkat
- Material Safety Data Sheet: 1. Chemical Product and Company IdentificationDokumen7 halamanMaterial Safety Data Sheet: 1. Chemical Product and Company IdentificationKun Adi ReksatamaBelum ada peringkat
- Fundamentals of Nursing10-19Dokumen19 halamanFundamentals of Nursing10-19escolarBelum ada peringkat
- Detailed Lesson Plan in Quarter 4 WK 1 Digestive ProcessDokumen10 halamanDetailed Lesson Plan in Quarter 4 WK 1 Digestive ProcessmalouBelum ada peringkat
- Berger 1986Dokumen3 halamanBerger 1986kameliasitorusBelum ada peringkat
- The Impact of Life Cycles on Family HealthDokumen27 halamanThe Impact of Life Cycles on Family Healthmarcial_745578124Belum ada peringkat
- TIME Magazine December 1Dokumen99 halamanTIME Magazine December 1rathneshkumar100% (2)
- Bacterial ReproductionDokumen12 halamanBacterial Reproductionchann.maahiBelum ada peringkat
- Types of Feeding TubesDokumen8 halamanTypes of Feeding TubesElda KuizonBelum ada peringkat
- AIPG Paper CorrectedDokumen42 halamanAIPG Paper CorrectedbrihaspathiacademyBelum ada peringkat
- Biochemistry Aspect in Human Reproduction: Lastri Mei WinarniDokumen19 halamanBiochemistry Aspect in Human Reproduction: Lastri Mei WinarniLastri Mei WinarniBelum ada peringkat
- Poodle Papers Spring 2004Dokumen36 halamanPoodle Papers Spring 2004PCA_website100% (6)
- Single Best Answer Question-Writing Tips For Clinicians: J L Walsh, B H L Harris, P E SmithDokumen6 halamanSingle Best Answer Question-Writing Tips For Clinicians: J L Walsh, B H L Harris, P E SmithSandro ToninBelum ada peringkat
- 2006 Human and Developmental Toxicology - D. Bellinger (Informa, 2006) WW PDFDokumen555 halaman2006 Human and Developmental Toxicology - D. Bellinger (Informa, 2006) WW PDFGiovana BarbosaBelum ada peringkat
- Word Parts Dictionary, Prefixes, Suffixes, Roots and Combining FormsDokumen237 halamanWord Parts Dictionary, Prefixes, Suffixes, Roots and Combining Formslaukings100% (9)
- Cronbachs AlphaDokumen2 halamanCronbachs AlphaSonia Ticona BenaventeBelum ada peringkat
- Internet Book of Critical Care (IBCC) : Rapid ReferenceDokumen1 halamanInternet Book of Critical Care (IBCC) : Rapid Referenceian porterBelum ada peringkat
- Lecture 12 Health Management Information SystemDokumen14 halamanLecture 12 Health Management Information SystemKamran SheikhBelum ada peringkat
- Nutritional Care in Respiratory Disease: DR Haerani Rasyid, Mkes, SPPD, K-GHDokumen94 halamanNutritional Care in Respiratory Disease: DR Haerani Rasyid, Mkes, SPPD, K-GHDesywinBelum ada peringkat
- A Concise Review On Nerium Oleander L.Dokumen5 halamanA Concise Review On Nerium Oleander L.tatralor100% (1)
- Understanding Cholesterol Levels and Risks: A Guide to Lipid ProfilesDokumen48 halamanUnderstanding Cholesterol Levels and Risks: A Guide to Lipid ProfilesAnonymous o3Q3QXEBelum ada peringkat
- Rectal Cancer,: Clinical Practice Guidelines in OncologyDokumen28 halamanRectal Cancer,: Clinical Practice Guidelines in OncologyRaíla SoaresBelum ada peringkat
- PEGS CatalogDokumen88 halamanPEGS CatalogMBelum ada peringkat
- Gtbr2016 Main TextDokumen214 halamanGtbr2016 Main TextRaimundo Isidro MachavaBelum ada peringkat
- Target Client List For NCD Prevention and Control SERVICES (Part 1)Dokumen9 halamanTarget Client List For NCD Prevention and Control SERVICES (Part 1)Lchg KrvyBelum ada peringkat
- Prevent HIV TransmissionDokumen6 halamanPrevent HIV TransmissionHazel EstayanBelum ada peringkat
- Tumor Detection Through Mri Brain Images: Rohit Arya 20MCS1009Dokumen25 halamanTumor Detection Through Mri Brain Images: Rohit Arya 20MCS1009Rohit AryaBelum ada peringkat
- Unit 7 Text QuestionsDokumen2 halamanUnit 7 Text QuestionsNiyanth RajaBelum ada peringkat
- Causes, Signs, and Treatment of HyponatremiaDokumen65 halamanCauses, Signs, and Treatment of HyponatremiaFaryalBalochBelum ada peringkat
- Nat Ag Winter Wheat in N Europe by Marc BonfilsDokumen5 halamanNat Ag Winter Wheat in N Europe by Marc BonfilsOrto di CartaBelum ada peringkat