Anda mungkin juga menyukai
- NCM 105 Notes 1Dokumen11 halamanNCM 105 Notes 1ApRil Anne BalanonBelum ada peringkat
- SYLLABUS PsycheDokumen39 halamanSYLLABUS PsycheRubz Bulquerin100% (1)
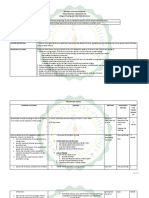
- CJL NCM 105 Obe Lec FinalDokumen11 halamanCJL NCM 105 Obe Lec FinalCarissa De Luzuriaga-BalariaBelum ada peringkat
- Professional Adjustment Final 2Dokumen41 halamanProfessional Adjustment Final 2lielani_martinezBelum ada peringkat
- Concepts On Mental Health IllnessDokumen13 halamanConcepts On Mental Health IllnessKoleen Lhyte UyBelum ada peringkat
- Nursing Theory Presentation2021Dokumen31 halamanNursing Theory Presentation2021Zistan HussienBelum ada peringkat
- Psychiatric Nursing Bullets 4Dokumen25 halamanPsychiatric Nursing Bullets 4winner gift flowersBelum ada peringkat
- NCM 108 Week 1 Topic 2 Part 2: International Code of Ethics For NursesDokumen4 halamanNCM 108 Week 1 Topic 2 Part 2: International Code of Ethics For NursesMarielle ChuaBelum ada peringkat
- Nle Test Plan For July 2012 Nle: Nursing Practice IDokumen7 halamanNle Test Plan For July 2012 Nle: Nursing Practice IPhilip AdallaBelum ada peringkat
- The Nursing ProcessDokumen9 halamanThe Nursing Processiannello100% (2)
- NCM 101 Endterm NotessssDokumen590 halamanNCM 101 Endterm NotessssJude Marie Claire DequiñaBelum ada peringkat
- Perception & Coordination NCM 104Dokumen162 halamanPerception & Coordination NCM 104bianqueeBelum ada peringkat
- Reviewer JonaidDokumen100 halamanReviewer JonaidjonaidtBelum ada peringkat
- Chapter 2 Lesson 4Dokumen3 halamanChapter 2 Lesson 4Myla Claire AlipioBelum ada peringkat
- Chapter 2 Lesson 1 and 2Dokumen14 halamanChapter 2 Lesson 1 and 22C1 - YABES, JenniferBelum ada peringkat
- PsychDokumen22 halamanPsychJonathan Q. ArancoBelum ada peringkat
- Psychiatric Nursing Handout 09-10 FCDokumen38 halamanPsychiatric Nursing Handout 09-10 FCAlvin Flores AbalosBelum ada peringkat
- Lesson Plan 5Dokumen3 halamanLesson Plan 5api-232466940Belum ada peringkat
- NCM 217 SKILLS LAB Maladpative Nursing 3Dokumen60 halamanNCM 217 SKILLS LAB Maladpative Nursing 3Sophia IbuyanBelum ada peringkat
- Chapter 1 - Health Care Delivery and Nursing PracticeDokumen4 halamanChapter 1 - Health Care Delivery and Nursing Practicejane amosBelum ada peringkat
- By: Catherine M. Souribio, R.NDokumen40 halamanBy: Catherine M. Souribio, R.NIsrael AgrisBelum ada peringkat
- Neurobiologic Theories and PsychopharmacologyDokumen2 halamanNeurobiologic Theories and Psychopharmacologymyer pasandalanBelum ada peringkat
- Psychiatric Nursing ReviewerDokumen7 halamanPsychiatric Nursing ReviewerJay Soriano0% (1)
- Cancer Burden: Global Picture. Number of New Cancer Cases (In Millions)Dokumen5 halamanCancer Burden: Global Picture. Number of New Cancer Cases (In Millions)Samantha BolanteBelum ada peringkat
- Eteeap - NCM 106 Page 1Dokumen5 halamanEteeap - NCM 106 Page 1Marisol Jane JomayaBelum ada peringkat
- FUNDA HAND-OUT - Nursing As A ProfessionDokumen7 halamanFUNDA HAND-OUT - Nursing As A ProfessionYsabel Francesca AbadBelum ada peringkat
- Process Recording With RubricDokumen8 halamanProcess Recording With RubricAndrew GarskeBelum ada peringkat
- Case Presentation Evaluation ToolDokumen2 halamanCase Presentation Evaluation ToolCharlie Cotoner FalgueraBelum ada peringkat
- Different Field of Nursing: Geronimo C. Burce JRDokumen44 halamanDifferent Field of Nursing: Geronimo C. Burce JRBiway RegalaBelum ada peringkat
- 1.1. Concept of ManDokumen27 halaman1.1. Concept of ManTrisha SabaBelum ada peringkat
- Ncm107 Summarization of MCNDokumen40 halamanNcm107 Summarization of MCNArlyn Faith AlvarezBelum ada peringkat
- Mental Health Nursing II NURS 2310: Unit 1 Basic Concepts of Mental Health and Mental IllnessDokumen41 halamanMental Health Nursing II NURS 2310: Unit 1 Basic Concepts of Mental Health and Mental IllnessRocky Domingo LazaroBelum ada peringkat
- Aklan Polytechnic College: Performance Rating ScaleDokumen3 halamanAklan Polytechnic College: Performance Rating ScaleShane DamianBelum ada peringkat
- NLE Flyer EditedDokumen2 halamanNLE Flyer EditedPeak Excellence BaguioBelum ada peringkat
- ReviewerDokumen10 halamanReviewerPatricia LoanzonBelum ada peringkat
- NCM 118Dokumen14 halamanNCM 118joan bagnateBelum ada peringkat
- University of The Philippines Manila Palo, LeyteDokumen27 halamanUniversity of The Philippines Manila Palo, LeyteAbigail BrillantesBelum ada peringkat
- 1 Gerontology Nursing Concepts: Gloria P. de Leon, RN, RM, ManDokumen211 halaman1 Gerontology Nursing Concepts: Gloria P. de Leon, RN, RM, ManJohanine VillasantiagoBelum ada peringkat
- Legal and Ethical Issues in Psychiatric NursingDokumen3 halamanLegal and Ethical Issues in Psychiatric Nursingkiran mahalBelum ada peringkat
- Course Outline Health AssessmentDokumen5 halamanCourse Outline Health AssessmentHAZEL RODA ESTORQUE100% (1)
- NCM 15-116 Psych Dida SyllabusDokumen9 halamanNCM 15-116 Psych Dida SyllabusMaam CatacutanBelum ada peringkat
- Expanded Program On ImmunizationDokumen15 halamanExpanded Program On ImmunizationReygie MarsadaBelum ada peringkat
- Janas PsychDokumen64 halamanJanas PsychJonalyn Chewacheo100% (1)
- Perioperative Nursing: Rose Delia P. Ocariza, RN, MANDokumen66 halamanPerioperative Nursing: Rose Delia P. Ocariza, RN, MANDeva HiyasBelum ada peringkat
- Fundamentals of Nursin Final Examination-Answer Keys (March 18,2013Dokumen13 halamanFundamentals of Nursin Final Examination-Answer Keys (March 18,2013marsan12Belum ada peringkat
- Compilation of Nursing Theories With Concept AnalyzationDokumen164 halamanCompilation of Nursing Theories With Concept AnalyzationPatrick PantuaBelum ada peringkat
- Introduction To Psychiatric-Mental Health NursingDokumen33 halamanIntroduction To Psychiatric-Mental Health NursingJoms DevanoBelum ada peringkat
- Psychiatric Nursing ReviewerDokumen46 halamanPsychiatric Nursing ReviewerDick Morgan Ferrer100% (1)
- CH 4 - Treatment Settings and Theraputic Programs-Test-Bank-Tank PDFDokumen14 halamanCH 4 - Treatment Settings and Theraputic Programs-Test-Bank-Tank PDFtimBelum ada peringkat
- Psychiatric Nursing Questions With RationaleDokumen8 halamanPsychiatric Nursing Questions With RationaleLes ChiensBelum ada peringkat
- Health Care Ethics.w1Dokumen10 halamanHealth Care Ethics.w1Roshin TejeroBelum ada peringkat
- CHN NotesDokumen7 halamanCHN NotesAnvi Turingan PedronanBelum ada peringkat
- COMPREHENSIVE NURSING ACHIEVEMENT TEST (RN): Passbooks Study GuideDari EverandCOMPREHENSIVE NURSING ACHIEVEMENT TEST (RN): Passbooks Study GuideBelum ada peringkat
- Assistant Director of Nursing Care: Passbooks Study GuideDari EverandAssistant Director of Nursing Care: Passbooks Study GuideBelum ada peringkat
- Navigating Long-Term Care - A Practical Approach for NursesDari EverandNavigating Long-Term Care - A Practical Approach for NursesBelum ada peringkat
- Basic Concepts in Psychiatric NursingDokumen11 halamanBasic Concepts in Psychiatric NursingMae DacerBelum ada peringkat
- Chapter 4 - Lecture Outline: Joyce Hammer 1/23/2018Dokumen5 halamanChapter 4 - Lecture Outline: Joyce Hammer 1/23/2018Melchor Felipe SalvosaBelum ada peringkat
- Tracer Study of SPC GRADUATES 2015-2016Dokumen18 halamanTracer Study of SPC GRADUATES 2015-2016Melchor Felipe Salvosa100% (1)
- Con Mission, Vision, ObjectivesDokumen1 halamanCon Mission, Vision, ObjectivesMelchor Felipe SalvosaBelum ada peringkat
- OBE Syllabus HA Summer 2014Dokumen16 halamanOBE Syllabus HA Summer 2014Melchor Felipe SalvosaBelum ada peringkat
- Tracer Study SPC GRADUATES 2015 and 2016Dokumen6 halamanTracer Study SPC GRADUATES 2015 and 2016Melchor Felipe SalvosaBelum ada peringkat
- Care of Mother, Child, Family and Population Group At-Risk or With ProblemsDokumen52 halamanCare of Mother, Child, Family and Population Group At-Risk or With ProblemsMelchor Felipe Salvosa100% (1)
- Micro OBSDokumen10 halamanMicro OBSMelchor Felipe SalvosaBelum ada peringkat
- Enrichment of The Outcomes-Based Education (Obe) Syllabus CON-School of Midwifery AY 2013-2014 First SemesterDokumen6 halamanEnrichment of The Outcomes-Based Education (Obe) Syllabus CON-School of Midwifery AY 2013-2014 First SemesterMelchor Felipe SalvosaBelum ada peringkat
- What Happens in The Operating RoomDokumen137 halamanWhat Happens in The Operating RoomMelchor Felipe Salvosa100% (1)
- NCM 106 Resource UnitDokumen15 halamanNCM 106 Resource UnitMelchor Felipe SalvosaBelum ada peringkat
- Homeostasis, Stress, and AdaptationDokumen16 halamanHomeostasis, Stress, and AdaptationMelchor Felipe SalvosaBelum ada peringkat
- Concept of Health and IllnessDokumen29 halamanConcept of Health and IllnessMelchor Felipe SalvosaBelum ada peringkat
- Chapter 7 - Lecture Outline Nursing Care of Clients Having SurgeryDokumen8 halamanChapter 7 - Lecture Outline Nursing Care of Clients Having SurgeryMelchor Felipe SalvosaBelum ada peringkat
- Beauty Pageant QuestionsDokumen14 halamanBeauty Pageant QuestionsMelchor Felipe Salvosa70% (10)
- San Pablo Colleges College of Nursing San Pablo City: Dr. Anita R. Rico 2011Dokumen1 halamanSan Pablo Colleges College of Nursing San Pablo City: Dr. Anita R. Rico 2011Melchor Felipe SalvosaBelum ada peringkat
- Spiritual Care NursingDokumen34 halamanSpiritual Care NursingMelchor Felipe SalvosaBelum ada peringkat
- NCM 102 LectureDokumen165 halamanNCM 102 LectureMelchor Felipe SalvosaBelum ada peringkat
- Alterations in OxygenationDokumen104 halamanAlterations in OxygenationMelchor Felipe Salvosa100% (1)
- Vital Signs Monitoring SheetDokumen2 halamanVital Signs Monitoring SheetMelchor Felipe SalvosaBelum ada peringkat
- Respiratory ModalitiesDokumen61 halamanRespiratory ModalitiesMelchor Felipe Salvosa100% (1)
- Self Suevey LIbrary AreaDokumen33 halamanSelf Suevey LIbrary AreaMelchor Felipe SalvosaBelum ada peringkat
- Immunology & Oncology Review 2Dokumen99 halamanImmunology & Oncology Review 2Melchor Felipe SalvosaBelum ada peringkat
- Philippines Point Grading SystemDokumen3 halamanPhilippines Point Grading SystemMelchor Felipe SalvosaBelum ada peringkat
- Outcomes Based SyllabusDokumen15 halamanOutcomes Based SyllabusMelchor Felipe SalvosaBelum ada peringkat
- APA FormatDokumen47 halamanAPA FormatMelchor Felipe SalvosaBelum ada peringkat
- Oncology Nursing LectureDokumen39 halamanOncology Nursing LectureMelchor Felipe SalvosaBelum ada peringkat
- HEALTH ETHICS Lecture 1Dokumen10 halamanHEALTH ETHICS Lecture 1Melchor Felipe Salvosa100% (1)
- Enrichment of The OBE SyllabusDokumen6 halamanEnrichment of The OBE SyllabusMelchor Felipe SalvosaBelum ada peringkat
- Beauty Pageant QuestionsDokumen14 halamanBeauty Pageant QuestionsMelchor Felipe Salvosa70% (10)
- Benign Malignant TableDokumen3 halamanBenign Malignant TableMelchor Felipe SalvosaBelum ada peringkat
- Assessing Scientist and Practitioner Orientations in Industrial/Organizational PsychologyDokumen17 halamanAssessing Scientist and Practitioner Orientations in Industrial/Organizational PsychologyRosaryco CG groupBelum ada peringkat
- List of Medical Professionals-SPADokumen8 halamanList of Medical Professionals-SPANoemí GuzmartBelum ada peringkat
- Sample Thesis Clinical PsychologyDokumen5 halamanSample Thesis Clinical Psychologypavopeikd100% (2)
- Test Bank For Counseling Children and Adolescents in Schools by Robyn S Hess Sandy Magnuson Linda M Mary BeelerDokumen35 halamanTest Bank For Counseling Children and Adolescents in Schools by Robyn S Hess Sandy Magnuson Linda M Mary Beelerbetwixtaft.1x1kk100% (45)
- Dissertation Ideas For Forensic PsychologyDokumen7 halamanDissertation Ideas For Forensic PsychologyPayForPaperCanada100% (1)
- Psychotherapy, OPQ, Bill 21 - Letter To Krystelle Larouche From Patricia Ivan (5-21-14)Dokumen3 halamanPsychotherapy, OPQ, Bill 21 - Letter To Krystelle Larouche From Patricia Ivan (5-21-14)PatriciaIvanBelum ada peringkat
- HB 9611 Psych ActDokumen19 halamanHB 9611 Psych ActLena BeeBelum ada peringkat
- What Is Clinical Psychology?: DefinitionsDokumen15 halamanWhat Is Clinical Psychology?: DefinitionsJay Mark CabreraBelum ada peringkat
- Castillo v. Republic Full CaseDokumen9 halamanCastillo v. Republic Full CaseQuiela QueenBelum ada peringkat
- Patterns of Psychologists Interprofessional Collaboration AcrossDokumen26 halamanPatterns of Psychologists Interprofessional Collaboration AcrossLNNGABelum ada peringkat
- School Psychologist ResumeDokumen8 halamanSchool Psychologist Resumefvntkabdf100% (2)
- 666Dokumen9 halaman666roselin sahayamBelum ada peringkat
- The Neurobiological Roots Of: Obsessive-Compulsive DisorderDokumen9 halamanThe Neurobiological Roots Of: Obsessive-Compulsive DisorderFaris Aziz PridiantoBelum ada peringkat
- Petts, Ann - Shapley, Bernard - On Supervision - Psychoanalytic and Jungian Analytic Perspectives-Karnac (2007)Dokumen266 halamanPetts, Ann - Shapley, Bernard - On Supervision - Psychoanalytic and Jungian Analytic Perspectives-Karnac (2007)Tiago AlvesBelum ada peringkat
- IO Psych in The PhilippinesDokumen3 halamanIO Psych in The Philippinesnauw zBelum ada peringkat
- Sport PsychologyDokumen7 halamanSport Psychologyapi-298900098Belum ada peringkat
- Feldmaneup14 PPT ch01 AccessibleDokumen72 halamanFeldmaneup14 PPT ch01 AccessibleSiraj KabbaraBelum ada peringkat
- Interview Assignment (Bi3)Dokumen8 halamanInterview Assignment (Bi3)UkhtiAizzahBelum ada peringkat
- Psychotherapy Definition, Goals and Stages of PsychotherapyDokumen5 halamanPsychotherapy Definition, Goals and Stages of PsychotherapycynthiasenBelum ada peringkat
- Work & Org Psych in Latin America IACCP2018Dokumen21 halamanWork & Org Psych in Latin America IACCP2018Kennedy AlecrimBelum ada peringkat
- School Psychologist Cover Letter ExampleDokumen8 halamanSchool Psychologist Cover Letter Exampledmipdsekg100% (1)
- All Department of Employemt and Labour VacanciesDokumen10 halamanAll Department of Employemt and Labour VacanciesAbundio O Pabe JrBelum ada peringkat
- Goodwin 2008Dokumen8 halamanGoodwin 2008GutoGonçalvesBelum ada peringkat
- Career DevelopmentDokumen26 halamanCareer DevelopmentAngeline ParadoBelum ada peringkat
- Praxis CBTinPractice ODCEpacketDokumen4 halamanPraxis CBTinPractice ODCEpacketJ.C. GarzaBelum ada peringkat
- Addressing Gaps in Mental Health Services For Older AdultsDokumen17 halamanAddressing Gaps in Mental Health Services For Older AdultsResidentes PsiquiatríaBelum ada peringkat
- Lec 1 105Dokumen70 halamanLec 1 105Melchor Felipe SalvosaBelum ada peringkat
- Sample Report PDFDokumen32 halamanSample Report PDFravibhargavaraamBelum ada peringkat
- Request Letter To PMODokumen4 halamanRequest Letter To PMONeeraj MishraBelum ada peringkat