Anda mungkin juga menyukai
- TPE Protocol 2018Dokumen5 halamanTPE Protocol 2018AnaBelum ada peringkat
- Major Haemorrhage ProtocolsDokumen3 halamanMajor Haemorrhage ProtocolsleicesterbugBelum ada peringkat
- Bleeding in A NeonateDokumen36 halamanBleeding in A NeonateDrBibek AgarwalBelum ada peringkat
- Malignant Hyperthermia PDFDokumen5 halamanMalignant Hyperthermia PDFKyla Barrera TabungarBelum ada peringkat
- 4 13 Transfusion of Blood ComponentsDokumen2 halaman4 13 Transfusion of Blood ComponentsAbu HuzaifaBelum ada peringkat
- Apheresis: by Ekta JajodiaDokumen54 halamanApheresis: by Ekta JajodiaMona YuliariBelum ada peringkat
- Prevention and Medical Management of Uterine Atony: by Cheong Lu Jeat, Laow Yee Kean Supervised by DR MunisDokumen17 halamanPrevention and Medical Management of Uterine Atony: by Cheong Lu Jeat, Laow Yee Kean Supervised by DR MunisCatherine PingBelum ada peringkat
- Rational Use of Safe BloodDokumen22 halamanRational Use of Safe Bloodkamnasharma0907Belum ada peringkat
- Emily Antes - 2018 Fall MeetDokumen41 halamanEmily Antes - 2018 Fall MeetSyed Shahrul Naz Syed100% (1)
- Pentostatin V4 6.14Dokumen2 halamanPentostatin V4 6.14GabrielBelum ada peringkat
- Blood Components - DR. ETU-EFEOTOR T. P.Dokumen40 halamanBlood Components - DR. ETU-EFEOTOR T. P.Princewill Seiyefa100% (1)
- Assessment and Concept Map Care Plan For Critical Care PatientDokumen11 halamanAssessment and Concept Map Care Plan For Critical Care Patientapi-604551723Belum ada peringkat
- Homologous Blood Trasfusion Practice ShortsDokumen23 halamanHomologous Blood Trasfusion Practice ShortsdrprasadingleyBelum ada peringkat
- Exchange TransfusionDokumen35 halamanExchange Transfusionsobinjohnpkl100% (2)
- TPE Guideline 2020Dokumen16 halamanTPE Guideline 2020Nedelcu CarmenBelum ada peringkat
- Complications Blood TransfusionDokumen7 halamanComplications Blood TransfusionWajeehaWasimBelum ada peringkat
- Blood and Blood Product (F)Dokumen50 halamanBlood and Blood Product (F)bharat singhBelum ada peringkat
- Blood Components Dosage and Their Administration (Compatibility Mode)Dokumen7 halamanBlood Components Dosage and Their Administration (Compatibility Mode)Chandra SekarBelum ada peringkat
- Blood and Blood ProductsDokumen52 halamanBlood and Blood Productswellawalalasith100% (1)
- Fresh Frozen Plasma (FFP)Dokumen1 halamanFresh Frozen Plasma (FFP)Prajatiya HarwokoBelum ada peringkat
- Massive Blood Loss Protocol AdultDokumen2 halamanMassive Blood Loss Protocol AdultNasif SadikBelum ada peringkat
- 05 Lanyard Cards - Blood Prescribing Card v3.2 FINALDokumen2 halaman05 Lanyard Cards - Blood Prescribing Card v3.2 FINALAbdul RaufBelum ada peringkat
- Pediatric Hematology Oncology Ward Officer HandbookDokumen40 halamanPediatric Hematology Oncology Ward Officer HandbookAnonymous FSUnLYr4yBelum ada peringkat
- UHP ROTEM ImplementationDokumen30 halamanUHP ROTEM Implementationppica8111Belum ada peringkat
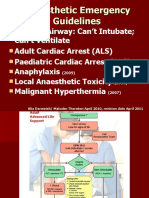
- Emergency GuidelinesDokumen11 halamanEmergency GuidelineswinstonappsBelum ada peringkat
- West Midlands Regional Training Package For Safe Blood Transfusion PracticeDokumen20 halamanWest Midlands Regional Training Package For Safe Blood Transfusion PracticeekramsBelum ada peringkat
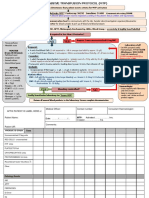
- Baseline:: Notify Transfusion Laboratory To: Activate MTP'. Footscray: 56292 Sunshine: 51480 Allocate Team RolesDokumen2 halamanBaseline:: Notify Transfusion Laboratory To: Activate MTP'. Footscray: 56292 Sunshine: 51480 Allocate Team RolesDumindu PereraBelum ada peringkat
- Blood and Blood ComponentsDokumen51 halamanBlood and Blood ComponentsMinlun ChongloiBelum ada peringkat
- Cross Cover Survival Guide: Electrolyte ReplacementDokumen5 halamanCross Cover Survival Guide: Electrolyte Replacementjrbull88Belum ada peringkat
- Canine Blood Component TableDokumen1 halamanCanine Blood Component TableTrifan PatriciaBelum ada peringkat
- Sample Ultrasound ReportDokumen3 halamanSample Ultrasound ReportPapadoveBelum ada peringkat
- Massive Haemorrhage PPT en PDFDokumen18 halamanMassive Haemorrhage PPT en PDFviaereaBelum ada peringkat
- Blood ProductsDokumen41 halamanBlood ProductsrijjorajooBelum ada peringkat
- Blood Component Therapy-4th Year MSDokumen22 halamanBlood Component Therapy-4th Year MSAyu Roossea MustikaBelum ada peringkat
- IV Push MedicationsDokumen67 halamanIV Push Medicationsbtalera100% (1)
- IRIS 2009 Treatment Recommendations SummaryDokumen5 halamanIRIS 2009 Treatment Recommendations SummaryJessicaHernandezBelum ada peringkat
- Hycamtin Epar Product Information - enDokumen59 halamanHycamtin Epar Product Information - enBRDBelum ada peringkat
- Management Protocol of Septic Shock: DiagnosisDokumen3 halamanManagement Protocol of Septic Shock: Diagnosissky nutsBelum ada peringkat
- Massive Blood TransfusionDokumen17 halamanMassive Blood TransfusionevanBelum ada peringkat
- Board Review HematologyDokumen30 halamanBoard Review HematologyPPDS Geriatri IPD UABelum ada peringkat
- BLOOD - FinalDokumen8 halamanBLOOD - FinalanuBelum ada peringkat
- Blood TransfusionDokumen18 halamanBlood TransfusionRheimon Jay Abuan BalcitaBelum ada peringkat
- Blood ComponentDokumen33 halamanBlood Componentmatrixtrinity100% (1)
- Hyperadrenocorticism: Cushing'S Disease: Clinical SignsDokumen4 halamanHyperadrenocorticism: Cushing'S Disease: Clinical Signsreerwrr qeqweBelum ada peringkat
- Blood Transfusion Peter HudsonDokumen21 halamanBlood Transfusion Peter HudsonWai YanBelum ada peringkat
- Anaestetic Management of Liver DiseaseDokumen86 halamanAnaestetic Management of Liver DiseaseVarun Reddy VBelum ada peringkat
- SCLC Cisplatin-Etoposide IVplusor-RT Protocol V1.1Dokumen3 halamanSCLC Cisplatin-Etoposide IVplusor-RT Protocol V1.1vera docBelum ada peringkat
- Massive Transfusion Protocol-BbhDokumen17 halamanMassive Transfusion Protocol-Bbhkrgdurai100% (1)
- Anticoagulation Protocol For PostDokumen8 halamanAnticoagulation Protocol For PostMohammed IbrahimBelum ada peringkat
- SC2 Sample Written Paper Questions With Answers 1Dokumen11 halamanSC2 Sample Written Paper Questions With Answers 1Zi SongBelum ada peringkat
- Disseminated Intravascular CoagulationDokumen37 halamanDisseminated Intravascular CoagulationhipoclaudioBelum ada peringkat
- Dr. Sunatrio - Management Hypovolemic ShockDokumen59 halamanDr. Sunatrio - Management Hypovolemic ShockArga Putra SaboeBelum ada peringkat
- Massive Transfusion ProtocolDokumen1 halamanMassive Transfusion ProtocoldraymanhussiennotionBelum ada peringkat
- FluidslectureDokumen26 halamanFluidslectureIgor StefanetBelum ada peringkat
- Disseminated Intravascular CoagulationDokumen37 halamanDisseminated Intravascular CoagulationMuhammad Adeeb100% (1)
- Exchange TransfusionDokumen9 halamanExchange TransfusiondewpraBelum ada peringkat
- Blood TransfusionDokumen65 halamanBlood TransfusionKate Lucernas MayugaBelum ada peringkat
- Blood Transfusion Therapy DefinitionDokumen27 halamanBlood Transfusion Therapy DefinitionEvangelin MelvinBelum ada peringkat
- The Spectrum of Amniotic Fluid Embolism: Is Intralipid the solution ?Dari EverandThe Spectrum of Amniotic Fluid Embolism: Is Intralipid the solution ?Belum ada peringkat
- St. Martin de Porres Catholic School: First Monthly Examination in Science 7Dokumen4 halamanSt. Martin de Porres Catholic School: First Monthly Examination in Science 7Wang Ming YaBelum ada peringkat
- Campus Ministry Office: St. Martin de Porres Catholic SchoolDokumen1 halamanCampus Ministry Office: St. Martin de Porres Catholic SchoolWang Ming YaBelum ada peringkat
- Yesha Reviewer 3rd MonthlyDokumen9 halamanYesha Reviewer 3rd MonthlyWang Ming YaBelum ada peringkat
- Conduct and Personality Evaluation Form EditedDokumen1 halamanConduct and Personality Evaluation Form EditedWang Ming YaBelum ada peringkat
- 11 Key Areas of Responsibility in NursingDokumen1 halaman11 Key Areas of Responsibility in NursingWang Ming YaBelum ada peringkat
- Chapter 1-Nature of PhilosophyDokumen35 halamanChapter 1-Nature of PhilosophyWang Ming Ya100% (4)
- Inflammatory DisturbancesDokumen63 halamanInflammatory DisturbancesWang Ming YaBelum ada peringkat
- Chapter 1-Musculoskeletal SystemDokumen113 halamanChapter 1-Musculoskeletal SystemWang Ming YaBelum ada peringkat
- QUESTIONS in Social Dimensions Let ReviewDokumen8 halamanQUESTIONS in Social Dimensions Let ReviewWang Ming Ya100% (3)
- Assessment of Community Health NeedsDokumen20 halamanAssessment of Community Health NeedsWang Ming YaBelum ada peringkat
- PanuluyanDokumen8 halamanPanuluyanWang Ming YaBelum ada peringkat
- Chapter 2-Basic Care and ComfortDokumen37 halamanChapter 2-Basic Care and ComfortWang Ming YaBelum ada peringkat
- Multiple Associated Anomalies in Patients of Duodenal Atresia: A Case SeriesDokumen2 halamanMultiple Associated Anomalies in Patients of Duodenal Atresia: A Case SeriesMuhammad Bilal MirzaBelum ada peringkat
- Qa Tables FinalDokumen11 halamanQa Tables Finalapi-337188982Belum ada peringkat
- Autism Spectrum DisorderDokumen13 halamanAutism Spectrum Disorderapi-283801172Belum ada peringkat
- Intermittent ExotropiaDokumen15 halamanIntermittent ExotropiakarenafiafiBelum ada peringkat
- Aniapravan 2020Dokumen2 halamanAniapravan 2020Marcos HernandezBelum ada peringkat
- Jurnal CT ScanDokumen9 halamanJurnal CT ScanPungki Putra TamaraBelum ada peringkat
- My Article B AngleDokumen4 halamanMy Article B AngleNiyati VerulkarBelum ada peringkat
- Patofisiologi EksimDokumen47 halamanPatofisiologi EksimDandy Abdi Cita GemilangBelum ada peringkat
- Ijpp 2003Dokumen280 halamanIjpp 2003G VenkateshBelum ada peringkat
- Bathing of Newborn ChecklistDokumen6 halamanBathing of Newborn ChecklistMhel MG0% (1)
- Atlas of Osteopathic TechniquesDokumen81 halamanAtlas of Osteopathic TechniquesDanieleBelum ada peringkat
- Atypical EclampsiaDokumen3 halamanAtypical EclampsiadianaristinugraheniBelum ada peringkat
- Chapter 28 - Ethical and Legal Issues in Intensive Care Unit - Nursing EthicsDokumen19 halamanChapter 28 - Ethical and Legal Issues in Intensive Care Unit - Nursing EthicsKumara guru SankarBelum ada peringkat
- Application Form For Ksharsutra Training ProgrammeDokumen5 halamanApplication Form For Ksharsutra Training ProgrammeKirankumar MutnaliBelum ada peringkat
- A Biometric Approach To Aesthetic Crown LengtheningDokumen11 halamanA Biometric Approach To Aesthetic Crown LengtheningpercycgBelum ada peringkat
- Administration of The Behavioral Pediatrics Feeding Assessment SCDokumen50 halamanAdministration of The Behavioral Pediatrics Feeding Assessment SCPaula Caceres RiveraBelum ada peringkat
- AACC 14 AbstractBook 1 CombinedDokumen282 halamanAACC 14 AbstractBook 1 CombinedRetni HamidahBelum ada peringkat
- Interproximal Height of BoneDokumen3 halamanInterproximal Height of Bonefinislux1Belum ada peringkat
- SUID PresentationDokumen195 halamanSUID PresentationJugoslavaIlankovićBelum ada peringkat
- Spina BifidaDokumen1 halamanSpina BifidaM Isyhaduul IslamBelum ada peringkat
- Phototherapy ChecklistDokumen2 halamanPhototherapy ChecklistMA. JIZELLE (CELSO) SINFUEGO100% (2)
- 0003489414532777Dokumen10 halaman0003489414532777Lilia ScutelnicBelum ada peringkat
- Plan ProposalDokumen3 halamanPlan Proposalapi-253764164Belum ada peringkat
- Hospital MedicineDokumen36 halamanHospital MedicineCarlos HernándezBelum ada peringkat
- FCPS Par2Dokumen6 halamanFCPS Par2drhirasalmanBelum ada peringkat
- Iugr & Iufd: Dr. Salwa NeyaziDokumen27 halamanIugr & Iufd: Dr. Salwa NeyaziTri Ujiana SejatiBelum ada peringkat
- Charge Nurse ResponsibilitiesDokumen4 halamanCharge Nurse ResponsibilitiesdocpanchuBelum ada peringkat
- Aminacid MetabolismDokumen84 halamanAminacid MetabolismAaronJose100% (1)
- Medication Calculation Examination Study Guide: IV CalculationsDokumen2 halamanMedication Calculation Examination Study Guide: IV Calculationswaqas_xsBelum ada peringkat
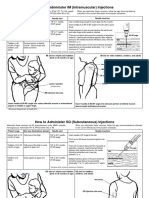
- Im SQ Admin PDFDokumen2 halamanIm SQ Admin PDFAlvin JjBelum ada peringkat