Anda mungkin juga menyukai
- Ocular EmergenciesDokumen26 halamanOcular EmergenciesYukianesa100% (1)
- Call ophthalmology immediately. Do not examine further or perform any procedures that could worsen injury. Cover eye securely and stabilizeDokumen32 halamanCall ophthalmology immediately. Do not examine further or perform any procedures that could worsen injury. Cover eye securely and stabilizenavenBelum ada peringkat
- Common Ocular EmergenciesDokumen33 halamanCommon Ocular EmergenciesMaimoona AimanBelum ada peringkat
- EYE DISORDERS: GLAUCOMA AND CATARACTSDokumen127 halamanEYE DISORDERS: GLAUCOMA AND CATARACTSjoan olanteBelum ada peringkat
- K.15 Ophtalmologic EmergenciesDokumen35 halamanK.15 Ophtalmologic EmergenciesZikri Putra Lan Lubis100% (1)
- Ophthalmology QuizDokumen45 halamanOphthalmology QuizLana LocoBelum ada peringkat
- Management of Ocular BurnsDokumen53 halamanManagement of Ocular BurnsPeter AbikoyeBelum ada peringkat
- OCULAR TRAUMA: SIGNS, SYMPTOMS AND MANAGEMENTDokumen50 halamanOCULAR TRAUMA: SIGNS, SYMPTOMS AND MANAGEMENTfatimaBelum ada peringkat
- Mira Ophth NotesDokumen27 halamanMira Ophth NotesMorticia AddamsBelum ada peringkat
- Glaucoma: Defitaria Permatasari I11109005Dokumen46 halamanGlaucoma: Defitaria Permatasari I11109005yusufharkianBelum ada peringkat
- Ocular EmergDokumen41 halamanOcular EmergMohd SyazrinBelum ada peringkat
- Emergency Eye Care WorkshopDokumen21 halamanEmergency Eye Care WorkshopAriani Ratri Dewi100% (1)
- Treat Ocular Emergencies FastDokumen29 halamanTreat Ocular Emergencies FastMohammad Farouq Omar100% (3)
- Glaucoma & CataractDokumen53 halamanGlaucoma & CataractBenita100% (1)
- Acute Glaucoma: Ni'Matul Muthmainnah I11111054Dokumen32 halamanAcute Glaucoma: Ni'Matul Muthmainnah I11111054Andari Putri WardhaniBelum ada peringkat
- UNIVERSITY OF MEDICAL SCIENCES"REZONANCA"-Halil Ajvazi/Ophthalmology/Prishtina/Republic of KosovaDokumen98 halamanUNIVERSITY OF MEDICAL SCIENCES"REZONANCA"-Halil Ajvazi/Ophthalmology/Prishtina/Republic of KosovaHALIL Z.AJVAZI100% (1)
- GlaucomaDokumen24 halamanGlaucomaRakeshBelum ada peringkat
- Glaucoma: Causes, Symptoms, Diagnosis and TreatmentDokumen52 halamanGlaucoma: Causes, Symptoms, Diagnosis and TreatmentIrfan SabirBelum ada peringkat
- By: Noor Majeed RehaniDokumen23 halamanBy: Noor Majeed RehaniMihaela TomaBelum ada peringkat
- Ocular Trauma 2021Dokumen63 halamanOcular Trauma 2021Fred PupeBelum ada peringkat
- Ocular Trauma Lecture MBBS by Prof Munim SuriDokumen60 halamanOcular Trauma Lecture MBBS by Prof Munim SuriMunim SuriBelum ada peringkat
- Impaired Vision and BlindnessDokumen44 halamanImpaired Vision and BlindnessYujenBelum ada peringkat
- Glaucoma: Zarieh Dawn Novela Medicine 2Dokumen41 halamanGlaucoma: Zarieh Dawn Novela Medicine 2Zari NovelaBelum ada peringkat
- 1 - Ocular TraumaDokumen31 halaman1 - Ocular TraumadeoshiBelum ada peringkat
- Ocular Injuries and EmergenciesDokumen60 halamanOcular Injuries and Emergenciesarnol3090100% (1)
- Gradual loss of vision-Nurses_065937Dokumen73 halamanGradual loss of vision-Nurses_065937CosbyBelum ada peringkat
- Trauma & Benda Asing Pada MataDokumen14 halamanTrauma & Benda Asing Pada MataTeguh Imana NugrahaBelum ada peringkat
- Ocular EmergDokumen61 halamanOcular EmergKBR RS UNHAS100% (1)
- Flashes and Floaters: Ahmed Shahab M08082Dokumen15 halamanFlashes and Floaters: Ahmed Shahab M08082Ahmed ShahabBelum ada peringkat
- Diseases of The Optic Nerve 09Dokumen25 halamanDiseases of The Optic Nerve 09somebody_maBelum ada peringkat
- Common Eye ConditionsDokumen35 halamanCommon Eye ConditionsElukoti BhosleBelum ada peringkat
- Optic Disc: Symptoms of The Optic Nerve DiseasesDokumen11 halamanOptic Disc: Symptoms of The Optic Nerve DiseasesDilawar JanBelum ada peringkat
- Central Serous Retinopathy PPT-2Dokumen28 halamanCentral Serous Retinopathy PPT-2Vaishu SgsBelum ada peringkat
- GlaucomeaDokumen21 halamanGlaucomeamalathiBelum ada peringkat
- Ocular Emergencies: Immediate TreatmentDokumen86 halamanOcular Emergencies: Immediate TreatmentBenny Franclin SuripattyBelum ada peringkat
- Lens DiseaseDokumen80 halamanLens Disease39 Akshit SetiaBelum ada peringkat
- Ophthalmology Neuro OphthalmologyDokumen7 halamanOphthalmology Neuro OphthalmologyjbtcmdtjjvBelum ada peringkat
- Chapter 11 Eye & Vision DisordersDokumen72 halamanChapter 11 Eye & Vision DisordersMYLENE GRACE ELARCOSABelum ada peringkat
- 6.GlaucomaDokumen52 halaman6.GlaucomacreativejoburgBelum ada peringkat
- Dr. Md. Yeamli Khan: Mbbs (Dhaka) Do (Du) Fcps (Ophth)Dokumen50 halamanDr. Md. Yeamli Khan: Mbbs (Dhaka) Do (Du) Fcps (Ophth)Kawshik SahaBelum ada peringkat
- Glaucoma: Seminar OnDokumen43 halamanGlaucoma: Seminar OnSanjay GarasiyaBelum ada peringkat
- Lecture 11 Special Senses Part 6-VisionDokumen48 halamanLecture 11 Special Senses Part 6-VisionMoses Jr KazevuBelum ada peringkat
- 03 Eyes and Ears 2 1Dokumen62 halaman03 Eyes and Ears 2 1Gerald BatugalBelum ada peringkat
- Optic Nerve PathologiesDokumen64 halamanOptic Nerve Pathologieshasan aslamBelum ada peringkat
- Optic Atrophy: Mshangila MD, M.MEDDokumen19 halamanOptic Atrophy: Mshangila MD, M.MEDCharles AnthonyBelum ada peringkat
- Eye Disorders Guide: Causes, Symptoms and Treatment of Cataracts and GlaucomaDokumen90 halamanEye Disorders Guide: Causes, Symptoms and Treatment of Cataracts and GlaucomaMonica JubaneBelum ada peringkat
- Ophthalmic EmergenciesDokumen25 halamanOphthalmic EmergenciesSameh AzizBelum ada peringkat
- Ocular Emergency: Dokter Muda Kevin Chikrista I4061172039Dokumen39 halamanOcular Emergency: Dokter Muda Kevin Chikrista I4061172039kevin chikristaBelum ada peringkat
- Glaucoma Guide: Types, Symptoms, Risks & TreatmentDokumen3 halamanGlaucoma Guide: Types, Symptoms, Risks & TreatmentplethoraldorkBelum ada peringkat
- Chronic Visual LossDokumen7 halamanChronic Visual LossJim Jose AntonyBelum ada peringkat
- Trauma and Ocular Emergencies: An OverviewDokumen35 halamanTrauma and Ocular Emergencies: An OverviewMochaLover100% (2)
- Glaucoma FinalDokumen40 halamanGlaucoma FinalAdoma SportsBelum ada peringkat
- Ataract Urgery: Reported By: Shane Ann Pedregosa BSN III-ADokumen20 halamanAtaract Urgery: Reported By: Shane Ann Pedregosa BSN III-AElex KimBelum ada peringkat
- Atrofia Nervului OpticDokumen23 halamanAtrofia Nervului OpticScerbatiuc CristinaBelum ada peringkat
- Gradual PAINLESS Diminution of Vision: By. Professor Sayed ElewahDokumen22 halamanGradual PAINLESS Diminution of Vision: By. Professor Sayed Elewahmrkhalid.sobhy67Belum ada peringkat
- ENT LESSON 8 (1)Dokumen45 halamanENT LESSON 8 (1)favourednancie9Belum ada peringkat
- Ophthalmology EmergenciesDokumen60 halamanOphthalmology Emergenciesasraf amirullahBelum ada peringkat
- Ophthalmology PDFDokumen28 halamanOphthalmology PDFKukuh Rizwido PrasetyoBelum ada peringkat
- Visual Field Loss in the Real World: A Book of Static Perimetry Test Targets for Eye Health ProfessionalsDari EverandVisual Field Loss in the Real World: A Book of Static Perimetry Test Targets for Eye Health ProfessionalsBelum ada peringkat
- Barriga V SB PDFDokumen2 halamanBarriga V SB PDFDarla GreyBelum ada peringkat
- 2016 Memo Circular No.19Dokumen42 halaman2016 Memo Circular No.19alicianatalialevisteBelum ada peringkat
- Remedial Law Cases With HighlightDokumen78 halamanRemedial Law Cases With HighlightAdrian HughesBelum ada peringkat
- Civil Law PDFDokumen9 halamanCivil Law PDFChanChi Domocmat LaresBelum ada peringkat
- Far East Shipping Co V CADokumen3 halamanFar East Shipping Co V CAJet Siang100% (1)
- SALES Memory AidDokumen39 halamanSALES Memory AidAgniezka AgniezkaBelum ada peringkat
- POEA SEC - 2010 AmendmentsDokumen37 halamanPOEA SEC - 2010 AmendmentsMark YfjBelum ada peringkat
- Writs and Criminal ProcedureDokumen14 halamanWrits and Criminal ProcedureJai CarungayBelum ada peringkat
- Bernas 903-924Dokumen22 halamanBernas 903-924Jai CarungayBelum ada peringkat
- Civil Law PDFDokumen9 halamanCivil Law PDFJai CarungayBelum ada peringkat
- 2014 Acute Pelvic PainDokumen74 halaman2014 Acute Pelvic PainJai CarungayBelum ada peringkat
- Inherent Factors Acquired Social/Environmental Factors Genetics Age Lifestyle DietDokumen1 halamanInherent Factors Acquired Social/Environmental Factors Genetics Age Lifestyle DietJai CarungayBelum ada peringkat
- SALES and LEASE Reviewer - DioryDokumen74 halamanSALES and LEASE Reviewer - DioryMaria Diory Rabajante95% (22)
- 2014 Jessup CompromisDokumen21 halaman2014 Jessup CompromisJohn Patrick CabreraBelum ada peringkat
- POEA SEC - 2010 AmendmentsDokumen37 halamanPOEA SEC - 2010 AmendmentsMark YfjBelum ada peringkat
- Land Acquisition OFWs.070605Dokumen5 halamanLand Acquisition OFWs.070605Jai CarungayBelum ada peringkat
- 2014 Acute Pelvic PainDokumen74 halaman2014 Acute Pelvic PainJai CarungayBelum ada peringkat
- CompromisDokumen67 halamanCompromisJai CarungayBelum ada peringkat
- 2014 Pediatric & Adolescent GynecologyDokumen77 halaman2014 Pediatric & Adolescent GynecologyJai CarungayBelum ada peringkat
- Busorg Case Digest CompilationDokumen56 halamanBusorg Case Digest CompilationJai CarungayBelum ada peringkat
- BusOrg Full Text Cases - 1st Case ListDokumen141 halamanBusOrg Full Text Cases - 1st Case ListJai CarungayBelum ada peringkat
- PIL Cases - 1st BatchDokumen47 halamanPIL Cases - 1st BatchJai CarungayBelum ada peringkat
- Ateneo 2007 Provrem-1Dokumen13 halamanAteneo 2007 Provrem-1Ljg BarondaBelum ada peringkat
- 2014 Acute Pelvic PainDokumen74 halaman2014 Acute Pelvic PainJai CarungayBelum ada peringkat
- Gel TechnologyDokumen2 halamanGel TechnologyJai Carungay100% (1)
- Petition CyberlawDokumen2 halamanPetition CyberlawJai CarungayBelum ada peringkat
- Management For Severe Acute BleedingDokumen1 halamanManagement For Severe Acute BleedingJai CarungayBelum ada peringkat
- 23 DieteticsDokumen71 halaman23 DieteticsJai CarungayBelum ada peringkat
- Criminal Procedure NotesDokumen37 halamanCriminal Procedure NotesJai CarungayBelum ada peringkat
- Cranial Nerve ExaminationDokumen3 halamanCranial Nerve Examinationapi-195986134Belum ada peringkat
- What Is Digital Image?: Remember Digitization Implies That A Digital Image Is An Approximation of A RealDokumen7 halamanWhat Is Digital Image?: Remember Digitization Implies That A Digital Image Is An Approximation of A RealBhagyesh ShahBelum ada peringkat
- 06 Refractive ErrorDokumen12 halaman06 Refractive ErrorMwanja MosesBelum ada peringkat
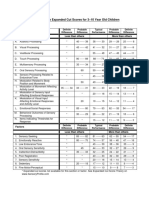
- Sensory Profile Expanded Cut Scores For 3-10 Year Old ChildrenDokumen1 halamanSensory Profile Expanded Cut Scores For 3-10 Year Old ChildrenAyra MagpiliBelum ada peringkat
- Circadian Field PhotometryDokumen80 halamanCircadian Field PhotometryMaría Ester Oyarzún GuzmánBelum ada peringkat
- MASTER'S GUIDE TO Manual SICSDokumen192 halamanMASTER'S GUIDE TO Manual SICSAndri SaputraBelum ada peringkat
- Glaucoma and Diabetes - Is There An Association? Jain Shashi, Lakhtakia Sujata, Tirkey Eva Rani, Jain Sheel ChandraDokumen5 halamanGlaucoma and Diabetes - Is There An Association? Jain Shashi, Lakhtakia Sujata, Tirkey Eva Rani, Jain Sheel ChandranjmdrBelum ada peringkat
- Detailed Lesson Plan No. 1Dokumen8 halamanDetailed Lesson Plan No. 1Pearl Agcopra100% (1)
- HDR CFA Image RenderingDokumen4 halamanHDR CFA Image RenderingJuanma FontBelum ada peringkat
- Classification of Age-Related CataractDokumen16 halamanClassification of Age-Related CataractDhea.MutiaraBelum ada peringkat
- Anatomy of The Eye PDFDokumen3 halamanAnatomy of The Eye PDFPerry SinBelum ada peringkat
- Visual Acuity: Presented By: Kartik Kumar Gupta G. Bhavani Reddy BV (Du) MC School of Optometry-2 YearDokumen61 halamanVisual Acuity: Presented By: Kartik Kumar Gupta G. Bhavani Reddy BV (Du) MC School of Optometry-2 Yearkartik GuptaBelum ada peringkat
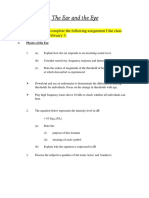
- The Physics of The Ear and Eye PDFDokumen3 halamanThe Physics of The Ear and Eye PDFNorctoic oneBelum ada peringkat
- Patient Instruction Guide: Vistakon (Etafilcon A) Contact LensesDokumen17 halamanPatient Instruction Guide: Vistakon (Etafilcon A) Contact LensessanieregianeeBelum ada peringkat
- Placement of Electrodes For: IFT by Prof Subin SolomenDokumen14 halamanPlacement of Electrodes For: IFT by Prof Subin SolomendvenumohanBelum ada peringkat
- AtropinDokumen36 halamanAtropintegarbondanBelum ada peringkat
- Examination of The Central Nervous SystemDokumen3 halamanExamination of The Central Nervous Systemkenners100% (13)
- Quick Guide to Tympanometry MeasurementsDokumen6 halamanQuick Guide to Tympanometry MeasurementsWilhelm HeinleinBelum ada peringkat
- Cranial Nerve Test & Testing KitsDokumen1 halamanCranial Nerve Test & Testing Kitsmamun31100% (1)
- Mod 19 Reading AssignmentDokumen2 halamanMod 19 Reading AssignmentDana M.Belum ada peringkat
- Ear Multiple ChoiceDokumen2 halamanEar Multiple Choicetano manoBelum ada peringkat
- Color Theory Lecture Topics for Principles of Visual Design 2720Dokumen233 halamanColor Theory Lecture Topics for Principles of Visual Design 2720bryanBelum ada peringkat
- Auditory Brainstem Evoked Response (Abr)Dokumen37 halamanAuditory Brainstem Evoked Response (Abr)Nitin Sharma100% (2)
- Noise Induced Hearing Loss EnglishDokumen4 halamanNoise Induced Hearing Loss EnglishReza SaputraBelum ada peringkat
- Dho Health Science Updated 8th Edition Simmers Test BankDokumen9 halamanDho Health Science Updated 8th Edition Simmers Test Bankjosephrodriguez04121993gbm100% (25)
- Four Major Divisions of Auditory System - AnatomyDokumen9 halamanFour Major Divisions of Auditory System - AnatomyJoshuaBelum ada peringkat
- RAAB Di IndonesiaDokumen42 halamanRAAB Di IndonesiaRaissa100% (2)
- Hearing Aids: For FamiliesDokumen25 halamanHearing Aids: For FamiliesNiharikaBelum ada peringkat
- UT Dallas Syllabus For hcs6332.001.07f Taught by (Otoole)Dokumen3 halamanUT Dallas Syllabus For hcs6332.001.07f Taught by (Otoole)UT Dallas Provost's Technology GroupBelum ada peringkat
- Dobesimi I Shikimit VISION LOSSDokumen7 halamanDobesimi I Shikimit VISION LOSSKreshnik HAJDARIBelum ada peringkat