Anda mungkin juga menyukai
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (120)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- PPSC Past Paper 2018 - Laiq Khan-1Dokumen14 halamanPPSC Past Paper 2018 - Laiq Khan-1Ali Arshad67% (3)
- Neuromuscular Blocking Agents: Suxamethonium (Succinylcholine)Dokumen5 halamanNeuromuscular Blocking Agents: Suxamethonium (Succinylcholine)Montaser BadranBelum ada peringkat
- Generic Price List (Aug'21)Dokumen24 halamanGeneric Price List (Aug'21)kiba elgibraBelum ada peringkat
- 1471 2458 13 367 PDFDokumen11 halaman1471 2458 13 367 PDFMagdalena PranataBelum ada peringkat
- Referat Kelompok 1 Uin (Rsko)Dokumen38 halamanReferat Kelompok 1 Uin (Rsko)Roysam AzmalBelum ada peringkat
- Case Kelompok 1 Uin (Rsko)Dokumen50 halamanCase Kelompok 1 Uin (Rsko)Roysam AzmalBelum ada peringkat
- Preceptor: Dr. Adhi Wibowo Nurhidayat, SPKJ, MPHDokumen50 halamanPreceptor: Dr. Adhi Wibowo Nurhidayat, SPKJ, MPHRoysam AzmalBelum ada peringkat
- Case Kelompok 1 Uin (Rsko)Dokumen50 halamanCase Kelompok 1 Uin (Rsko)Roysam AzmalBelum ada peringkat
- Laporan Home Visit Kelompok 1 Uin (Rsko)Dokumen18 halamanLaporan Home Visit Kelompok 1 Uin (Rsko)Roysam AzmalBelum ada peringkat
- Triamcinolone (Topical) - Drug InformationDokumen5 halamanTriamcinolone (Topical) - Drug InformationMauricio Sv0% (1)
- DSP 02 Juli 2022Dokumen32 halamanDSP 02 Juli 2022Pa RusdiyatBelum ada peringkat
- List-Of-Students For F2F ClassDokumen4 halamanList-Of-Students For F2F Classjoan marie PeliasBelum ada peringkat
- Prodrugs - Design and Clinical ApplicationsDokumen16 halamanProdrugs - Design and Clinical ApplicationsBlackbeatle63Belum ada peringkat
- FDC Guidelines - Revised1Dokumen38 halamanFDC Guidelines - Revised1gpg19751215Belum ada peringkat
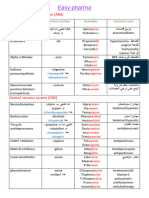
- Othmani111n Easy Pharma - 220401 - 163518Dokumen7 halamanOthmani111n Easy Pharma - 220401 - 163518Hassan HekmatBelum ada peringkat
- Respirology Case Reports: Paradoxical Bronchospasm: A Rare Adverse Effect of Fenoterol UseDokumen4 halamanRespirology Case Reports: Paradoxical Bronchospasm: A Rare Adverse Effect of Fenoterol UseDELLA LESTARIBelum ada peringkat
- Surat Pesanan Obat Apotek Ym 123Dokumen4 halamanSurat Pesanan Obat Apotek Ym 123ymBelum ada peringkat
- Rekap PBF 22-06-22Dokumen68 halamanRekap PBF 22-06-22SELVIABelum ada peringkat
- LovenoxDokumen1 halamanLovenoxAdrianne BazoBelum ada peringkat
- IOM Pharmacology IDokumen93 halamanIOM Pharmacology ISahara MahatBelum ada peringkat
- Drug Alert List of Oct - 2022Dokumen11 halamanDrug Alert List of Oct - 2022Gopal RaoBelum ada peringkat
- Simple Magazine #17Dokumen5 halamanSimple Magazine #17tôn thất minh khangBelum ada peringkat
- IMS Biosimilar 2017 - V9 PDFDokumen33 halamanIMS Biosimilar 2017 - V9 PDFPamela Ruiz RuizBelum ada peringkat
- Dokumen - Tips - Indeks Obat HewanDokumen36 halamanDokumen - Tips - Indeks Obat HewanSartine AurellioneBelum ada peringkat
- Classification and Pharmacology of ProgestinsDokumen10 halamanClassification and Pharmacology of ProgestinsancaBelum ada peringkat
- DM AAFP ManagementDokumen8 halamanDM AAFP ManagementphilsguBelum ada peringkat
- Tempelan ObatDokumen12 halamanTempelan Obatagus sulistyono SulistyonoBelum ada peringkat
- Antiemetics & Oral Rehydration Salts (ORS)Dokumen60 halamanAntiemetics & Oral Rehydration Salts (ORS)Saha DirllahBelum ada peringkat
- Anca VasculitisDokumen12 halamanAnca Vasculitisatul_desai_3100% (2)
- 627 1196 1 PBDokumen7 halaman627 1196 1 PBannisa dian zizianiBelum ada peringkat
- Word Cdi 7Dokumen7 halamanWord Cdi 7Yani100% (1)
- Illegal DrugsDokumen37 halamanIllegal Drugsangker arnelBelum ada peringkat
- Daftar Obat Prak 2Dokumen3 halamanDaftar Obat Prak 2Riza AsariBelum ada peringkat
- 508-Prowell-Final Slides5Dokumen25 halaman508-Prowell-Final Slides5dfsdjgflksjgnawBelum ada peringkat
- Alvogen Response BriefDokumen77 halamanAlvogen Response BriefM.H.Belum ada peringkat
- Part Two ResourcesDokumen4 halamanPart Two Resourcesapi-158169273Belum ada peringkat