Anda mungkin juga menyukai
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Gestational Trophoblastic NeoplasmDokumen21 halamanGestational Trophoblastic NeoplasmravannofanizzaBelum ada peringkat
- Periodeapril2015 PDFDokumen3 halamanPeriodeapril2015 PDFMarlinawatyBelum ada peringkat
- Daftar Isi GinekDokumen3 halamanDaftar Isi GinekravannofanizzaBelum ada peringkat
- GestosisDokumen12 halamanGestosisravannofanizzaBelum ada peringkat
- Daftar Isi GinekDokumen3 halamanDaftar Isi GinekravannofanizzaBelum ada peringkat
- Infeksi Torch Pada KehamilanDokumen54 halamanInfeksi Torch Pada KehamilanravannofanizzaBelum ada peringkat
- 96 FullDokumen14 halaman96 FullravannofanizzaBelum ada peringkat
- Headache: Henny Anggraini SadeliDokumen48 halamanHeadache: Henny Anggraini SadeliravannofanizzaBelum ada peringkat
- Monitoring HemodinamikDokumen60 halamanMonitoring HemodinamikravannofanizzaBelum ada peringkat
- Dnternational Federation of Gynecology and Obstetrics Staging of Endometrial CancerDokumen4 halamanDnternational Federation of Gynecology and Obstetrics Staging of Endometrial CancerravannofanizzaBelum ada peringkat
- RjpoDokumen11 halamanRjporavannofanizzaBelum ada peringkat
- Module of Skill Laboratorium PracticeDokumen44 halamanModule of Skill Laboratorium PracticeravannofanizzaBelum ada peringkat
- Radiologi Ileus Obstruksi Dan Ileus ParalitikDokumen18 halamanRadiologi Ileus Obstruksi Dan Ileus ParalitikravannofanizzaBelum ada peringkat
- Coma S1Dokumen37 halamanComa S1Egi Patnialdi Firda PermanaBelum ada peringkat
- 2.kuliah Sensoris 2006Dokumen42 halaman2.kuliah Sensoris 2006ravannofanizzaBelum ada peringkat
- Clinical of StrokeDokumen31 halamanClinical of StrokeIlham riandaBelum ada peringkat
- Basal Ganglia & Degenerative DisordersDokumen46 halamanBasal Ganglia & Degenerative DisordersRidha Surya NugrahaBelum ada peringkat
- Css Edema IntersitialDokumen21 halamanCss Edema IntersitialravannofanizzaBelum ada peringkat
- Css - CT Scan NormalDokumen16 halamanCss - CT Scan NormalravannofanizzaBelum ada peringkat
- Cerebral PalsyDokumen31 halamanCerebral PalsyravannofanizzaBelum ada peringkat
- AntiemeticDokumen36 halamanAntiemeticravannofanizza100% (1)
- RjpoDokumen11 halamanRjporavannofanizzaBelum ada peringkat
- Cerebral PalsyDokumen95 halamanCerebral Palsyravannofanizza100% (1)
- Cerebral PalsyDokumen14 halamanCerebral Palsyمحمد آدي نور أنور100% (1)
- Cerebral PalsyDokumen40 halamanCerebral PalsyravannofanizzaBelum ada peringkat
- Cerebral Palsy The ABC's: of CPDokumen43 halamanCerebral Palsy The ABC's: of CPravannofanizzaBelum ada peringkat
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Management of CoughDokumen54 halamanManagement of CoughNabilah AnandaBelum ada peringkat
- Drugs Study ER LEAD Drug (Yntig)Dokumen5 halamanDrugs Study ER LEAD Drug (Yntig)Herbert Almendras HuyoBelum ada peringkat
- Aspartame BrochureDokumen15 halamanAspartame BrochureBern KruijtBelum ada peringkat
- HHS Public AccessDokumen16 halamanHHS Public AccessintanBelum ada peringkat
- BooksDokumen5 halamanBooksDanijela VukcevicBelum ada peringkat
- IVD Medical Device V2Dokumen44 halamanIVD Medical Device V2Vadi VelanBelum ada peringkat
- The Aptitude HandbookDokumen295 halamanThe Aptitude HandbookSomesh SharmaBelum ada peringkat
- Summative Assessment - I English Communicative Cbse Class IxDokumen11 halamanSummative Assessment - I English Communicative Cbse Class Ixnaveen_halkBelum ada peringkat
- Health Beliefs in Bali SlidesDokumen18 halamanHealth Beliefs in Bali SlidesAwik WardaniBelum ada peringkat
- Aragwadha Virechan For LeprosyDokumen25 halamanAragwadha Virechan For LeprosyVaidya NurBelum ada peringkat
- Sample of Psychological ReportDokumen4 halamanSample of Psychological ReportRochelle Joyce Olmilla Bersamin67% (3)
- Efficacy of Nerve Flossing Technique On Improving Sciatic Nerve Function in Patients With Sciatica - A Randomized Controlled TrialDokumen10 halamanEfficacy of Nerve Flossing Technique On Improving Sciatic Nerve Function in Patients With Sciatica - A Randomized Controlled Trialsphadungkit100% (1)
- Multiple SclerosisDokumen96 halamanMultiple SclerosisDrGasnasBelum ada peringkat
- ChoreaDokumen4 halamanChoreaapi-19973386Belum ada peringkat
- (Final Proposal) 20181220 Beauttah Migiro Akuma - Research Proposal - Right To Health - Version 1.0Dokumen14 halaman(Final Proposal) 20181220 Beauttah Migiro Akuma - Research Proposal - Right To Health - Version 1.0Brian BeauttahBelum ada peringkat
- Hemophilia: Factor IX (Hemophilia B)Dokumen38 halamanHemophilia: Factor IX (Hemophilia B)Jhvhjgj JhhgtyBelum ada peringkat
- Manila Central University College of Medicine Department of PediatricsDokumen7 halamanManila Central University College of Medicine Department of PediatricsKirstie de LunaBelum ada peringkat
- HIV & TBDokumen51 halamanHIV & TBRhea DerijeBelum ada peringkat
- StrabismusDokumen20 halamanStrabismusmerycoBelum ada peringkat
- R7 US CatalogDokumen476 halamanR7 US CatalogmatzoneBelum ada peringkat
- Formation of Faeces and DefaecationDokumen15 halamanFormation of Faeces and Defaecationzurich100% (5)
- Intake and OutputDokumen3 halamanIntake and Outputtina100% (1)
- Quoting Sources Thetsane 2012Dokumen12 halamanQuoting Sources Thetsane 2012Teboho J MncinaBelum ada peringkat
- H3C Abstract Final 11262014Dokumen204 halamanH3C Abstract Final 11262014AAPI ConventionBelum ada peringkat
- Quantitative Estimation of Phytoconstituents of Caesalpinia PulcherrimaDokumen5 halamanQuantitative Estimation of Phytoconstituents of Caesalpinia PulcherrimaSriArthiBelum ada peringkat
- Pacificgoldenplover Microbe Mission Practice TestDokumen5 halamanPacificgoldenplover Microbe Mission Practice TestsandeeptaraBelum ada peringkat
- Magnesium Nitrate HexahydrateDokumen4 halamanMagnesium Nitrate HexahydrateCarmen M AvinazarBelum ada peringkat
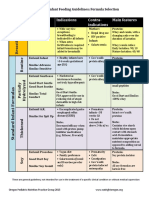
- Formula Selection OPNPGDokumen2 halamanFormula Selection OPNPGRina PratiwiBelum ada peringkat
- Directions: Choose The Letter of The Correct Answer. Write Your Answer On A Separate Sheet. STRICTLY NO Erasures and Write Capital Letters Only!Dokumen3 halamanDirections: Choose The Letter of The Correct Answer. Write Your Answer On A Separate Sheet. STRICTLY NO Erasures and Write Capital Letters Only!Diane CiprianoBelum ada peringkat
- KJO2086Dokumen13 halamanKJO2086jieunBelum ada peringkat