Anda mungkin juga menyukai
- TB Paru FK UncenDokumen66 halamanTB Paru FK UncenAndira Trianingrum TukanBelum ada peringkat
- PDF Makalah Stunting - CompressDokumen22 halamanPDF Makalah Stunting - CompressHusni TamrinBelum ada peringkat
- Syphilis CongenitalDokumen5 halamanSyphilis CongenitalElisse StephanieBelum ada peringkat
- Nephrotic Syndrome in Children: Supervised By: Dr. Pulung M. Silalahi Sp.A Presented By: Anna ListianaDokumen38 halamanNephrotic Syndrome in Children: Supervised By: Dr. Pulung M. Silalahi Sp.A Presented By: Anna ListianaAnna ListianaBelum ada peringkat
- Mims Indonesia - April.2017.en - SampleDokumen958 halamanMims Indonesia - April.2017.en - SampleAdetia MaharaniBelum ada peringkat
- Jurnal Reading Kulit (Jenifer Johana Paath 201383019)Dokumen34 halamanJurnal Reading Kulit (Jenifer Johana Paath 201383019)Mega BagdadBelum ada peringkat
- LEaflet TBCDokumen3 halamanLEaflet TBCatik mayasariBelum ada peringkat
- Dr. Bambang Pujo Semedi, SP An - Antibiotics in Critically Ill E4ED FinalDokumen46 halamanDr. Bambang Pujo Semedi, SP An - Antibiotics in Critically Ill E4ED FinalcittaarunikaBelum ada peringkat
- CSS TuberkulosisDokumen69 halamanCSS TuberkulosisdhaniBelum ada peringkat
- The Effectiveness of Galactomyces FermentDokumen6 halamanThe Effectiveness of Galactomyces FermentFransiscus Clinton100% (1)
- Program Book Online INDEPTH 2023 - 3Dokumen37 halamanProgram Book Online INDEPTH 2023 - 3George SitanayaBelum ada peringkat
- Bronko PneumoniaDokumen34 halamanBronko PneumoniaDippos Theofilus HBelum ada peringkat
- No. TGL Materi: Rehabilitation of Cardiovascular and Respiratory DisorderDokumen6 halamanNo. TGL Materi: Rehabilitation of Cardiovascular and Respiratory DisorderFatimah AzzahraBelum ada peringkat
- Definisi - Tatalaksana Terkini Tuberkulosis (TB) Dan TB-MDR: Fathiyah IsbaniahDokumen48 halamanDefinisi - Tatalaksana Terkini Tuberkulosis (TB) Dan TB-MDR: Fathiyah IsbaniahMagista NugrahaBelum ada peringkat
- Antibiotik Bijak Di RS - Dr. Ronald Irwanto Natadidjaja, SpPD-KPTI, FINASIMDokumen46 halamanAntibiotik Bijak Di RS - Dr. Ronald Irwanto Natadidjaja, SpPD-KPTI, FINASIMdeviamufidazBelum ada peringkat
- CDK Edisi CME-2 TH 2020 5 SKP PDFDokumen24 halamanCDK Edisi CME-2 TH 2020 5 SKP PDFnarinaaviBelum ada peringkat
- Hubungan Antara TB Dan HIVDokumen52 halamanHubungan Antara TB Dan HIVNurlaela Eka RostariBelum ada peringkat
- Erwin - Antibiotic Stewardship Program - PRAUD IIIDokumen11 halamanErwin - Antibiotic Stewardship Program - PRAUD IIIWidya Lestari CapawatyBelum ada peringkat
- Clinikal Pathway PDDokumen14 halamanClinikal Pathway PDIntan OktarinaBelum ada peringkat
- Seminar ISTC TB Feb 2016Dokumen12 halamanSeminar ISTC TB Feb 2016christine nathalia loupattyBelum ada peringkat
- Jurnal ObesitasDokumen7 halamanJurnal ObesitasOvieDaniaBelum ada peringkat
- Daftar Ebook THTDokumen3 halamanDaftar Ebook THTPrathita AmandaBelum ada peringkat
- Anti BiotikDokumen82 halamanAnti BiotikKaniaArfianiBelum ada peringkat
- Pemeriksaan Bakteriologis Lab TBDokumen49 halamanPemeriksaan Bakteriologis Lab TBTugas HeinzBelum ada peringkat
- Skripsi KustaDokumen61 halamanSkripsi Kustaandre yuindartantoBelum ada peringkat
- Manajemen Risiko Rca Fmea - 2Dokumen54 halamanManajemen Risiko Rca Fmea - 2Dwi Supma Bintara0% (1)
- Artikel Review Dermatitis AtopikDokumen8 halamanArtikel Review Dermatitis AtopikputriBelum ada peringkat
- Manifestasi Klinis Dan Penanganan Demam Berdarah Dengue Grade 1: Sebuah Tinjauan PustakaDokumen5 halamanManifestasi Klinis Dan Penanganan Demam Berdarah Dengue Grade 1: Sebuah Tinjauan Pustakanur aisyahBelum ada peringkat
- Analisis Pelayanan Terapeutik Pada Pasien Tuberkulosis Resisten Obat Di Kota MedanDokumen14 halamanAnalisis Pelayanan Terapeutik Pada Pasien Tuberkulosis Resisten Obat Di Kota MedanwahyuBelum ada peringkat
- Dr. Uun Sumardi, SPPD, K-PTI, KIC, FINASIM-Fluid Management in Severe DengueDokumen20 halamanDr. Uun Sumardi, SPPD, K-PTI, KIC, FINASIM-Fluid Management in Severe DengueOlivia DwimaswastiBelum ada peringkat
- Farmako Obat Anti HipertensiDokumen21 halamanFarmako Obat Anti HipertensiEka FitriBelum ada peringkat
- Pengenalan Icd-10 Struktur & IsiDokumen15 halamanPengenalan Icd-10 Struktur & IsiL. JamilBelum ada peringkat
- Bimbingan IMO UroreproDokumen12 halamanBimbingan IMO UroreproFatimah AzzahraBelum ada peringkat
- Nutrisi Dan Gizi BurukDokumen9 halamanNutrisi Dan Gizi BurukFifin HestiBelum ada peringkat
- Program Pengendalian Resistensi Antimikroba Di Rumah SakitDokumen23 halamanProgram Pengendalian Resistensi Antimikroba Di Rumah SakitYulia Wati Safitri SanjayaBelum ada peringkat
- Morbus HansenDokumen37 halamanMorbus HansenYolanda Agnesia Purba100% (1)
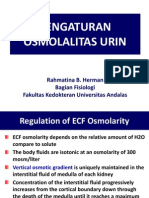
- Kuliah 3. Pengaturan Osmolalitas UrinDokumen19 halamanKuliah 3. Pengaturan Osmolalitas UrinAnnisa DamayantiBelum ada peringkat
- Diagnosis Dan Tatalaksana Tuberkulosis: Dr. DR Erlina Burhan Msc. SP.P (K)Dokumen44 halamanDiagnosis Dan Tatalaksana Tuberkulosis: Dr. DR Erlina Burhan Msc. SP.P (K)Laboratorium Ansari SalehBelum ada peringkat
- Otitis Media AkutDokumen31 halamanOtitis Media AkutNin DuskBelum ada peringkat
- TB Update 2016Dokumen67 halamanTB Update 2016Nila hermawatiBelum ada peringkat
- P-Drug FK UmmDokumen424 halamanP-Drug FK UmmsaidahrahmatBelum ada peringkat
- PPK Gagal Jantung AkutDokumen3 halamanPPK Gagal Jantung AkutIzzatun NisaBelum ada peringkat
- Monkey Pox Cacar Monyet: Dr. Cita BudiartiDokumen46 halamanMonkey Pox Cacar Monyet: Dr. Cita Budiarticita budiarti100% (1)
- FIXED DRUG ERUPTION PrintDokumen17 halamanFIXED DRUG ERUPTION PrintnajwaBelum ada peringkat
- Proses Pengembangan Vaksin Covid-19Dokumen27 halamanProses Pengembangan Vaksin Covid-19faluviekadianiBelum ada peringkat
- Primary Dysmenorrhea ConsensusDokumen11 halamanPrimary Dysmenorrhea ConsensusNorman AjxBelum ada peringkat
- Obat Antijamur: Wening Sari, DR., M.KesDokumen18 halamanObat Antijamur: Wening Sari, DR., M.KesdebbyelviraBelum ada peringkat
- Antimicrobial Stewardship ProgrammeDokumen12 halamanAntimicrobial Stewardship ProgrammeDesmiyati AdoeBelum ada peringkat
- Seboroik DermatitisDokumen21 halamanSeboroik DermatitisPutri PelealuBelum ada peringkat
- Proposal LPJ SumdokDokumen25 halamanProposal LPJ SumdokLasta ArshintaBelum ada peringkat
- Kapita Selekta: Haryati Bagian Penyakit Paru FK Unlam-RSU D UlinDokumen45 halamanKapita Selekta: Haryati Bagian Penyakit Paru FK Unlam-RSU D UlinM. Ridho Bagus PratamaBelum ada peringkat
- 12.uji Tuberkulin Dan Pencegahan TB Pada AnakDokumen29 halaman12.uji Tuberkulin Dan Pencegahan TB Pada AnakAndriano Arie WibowoBelum ada peringkat
- Uji Tuberkulin Dan Pencegahan TB Pada Anak: Ketikan Kuliah DR - Finny Fitry Yani, Sp.ADokumen29 halamanUji Tuberkulin Dan Pencegahan TB Pada Anak: Ketikan Kuliah DR - Finny Fitry Yani, Sp.AAndriano Arie WibowoBelum ada peringkat
- TuberculosisDokumen35 halamanTuberculosisAmr KhayyalBelum ada peringkat
- Diagnosis TBDokumen44 halamanDiagnosis TBGede Eka Putra NugrahaBelum ada peringkat
- Tuberculosis: Yang YuxiaDokumen126 halamanTuberculosis: Yang Yuxiaapi-19916399Belum ada peringkat
- Tuberculosis Unit 1 Lecture - 1Dokumen39 halamanTuberculosis Unit 1 Lecture - 1Kubra Rasool100% (1)
- Lopez, Marian Manuson, Ludy Melu, Anna Victoria Modina, Jayson Montenegro, Matilde Krisha 4dpharmacyDokumen19 halamanLopez, Marian Manuson, Ludy Melu, Anna Victoria Modina, Jayson Montenegro, Matilde Krisha 4dpharmacyRyan100% (1)
- TBC Presentation by CindyDokumen21 halamanTBC Presentation by Cindycindydenti54Belum ada peringkat
- Department of Child Health Faculty of Medicine University of Syiah KualaDokumen55 halamanDepartment of Child Health Faculty of Medicine University of Syiah KualaIrfandy Chairi Sulaiman LubisBelum ada peringkat
- Tugas Refleksi Kasus Kumpul Besok222Dokumen50 halamanTugas Refleksi Kasus Kumpul Besok222Ray SadisBelum ada peringkat
- Trauma ThoraxDokumen76 halamanTrauma ThoraxRay SadisBelum ada peringkat
- Curiculum Vitae DR Julie D BarlianaDokumen1 halamanCuriculum Vitae DR Julie D BarlianaRay SadisBelum ada peringkat
- Excel Hasil PenelitianDokumen5 halamanExcel Hasil PenelitianRay SadisBelum ada peringkat
- Pigmentation DisorderDokumen7 halamanPigmentation DisorderRay Sadis100% (1)
- 2010 American Heart Association Guidelines For Cardiopulmonary Resuscitation and Emergency Cardiovascular CareDokumen28 halaman2010 American Heart Association Guidelines For Cardiopulmonary Resuscitation and Emergency Cardiovascular CareRay SadisBelum ada peringkat
- Trauma ThoraxDokumen76 halamanTrauma ThoraxRay SadisBelum ada peringkat
- JR Radio MayshiaDokumen15 halamanJR Radio MayshiaRay SadisBelum ada peringkat
- Basis Neurobiologi DepresiDokumen24 halamanBasis Neurobiologi DepresiRay SadisBelum ada peringkat
- Basis Neurobiologi DepresiDokumen24 halamanBasis Neurobiologi DepresiRay SadisBelum ada peringkat
- Sudden Infat Death Syndrome: DR Landelina Lany T, Sp.A Rsu Kanujoso Djatiwibowo BalikpapanDokumen12 halamanSudden Infat Death Syndrome: DR Landelina Lany T, Sp.A Rsu Kanujoso Djatiwibowo BalikpapanRay SadisBelum ada peringkat
- Bipolar: Oleh: Jaya MualiminDokumen58 halamanBipolar: Oleh: Jaya MualiminRay Sadis100% (2)
- Farmakoterapi Pada KehamilanDokumen19 halamanFarmakoterapi Pada KehamilanRay SadisBelum ada peringkat
- PneumothoraxDokumen4 halamanPneumothoraxRay SadisBelum ada peringkat
- Guillain-Barré Syndrome (GBS) and Antecedent Campylobacter InfectionDokumen24 halamanGuillain-Barré Syndrome (GBS) and Antecedent Campylobacter InfectionRay SadisBelum ada peringkat
- Multiple TraumaDokumen17 halamanMultiple TraumaRay SadisBelum ada peringkat
- Endokrinologi, DR NoviaDokumen73 halamanEndokrinologi, DR NoviaSabila WahdiniBelum ada peringkat
- Blood Group Incompatibility RH DiseaseDokumen35 halamanBlood Group Incompatibility RH DiseaseRay SadisBelum ada peringkat
- Surgical InstrumentsDokumen78 halamanSurgical InstrumentsPriyanka VishwakarmaBelum ada peringkat
- Hubungan Hipertensi Dan Glycohemoglobin (Hba1c) Dengan Kejadian Retinopati Diabetik Pada Penderita Diabetes Melitus Di Rsud Margono Soekarjo PurwokertoDokumen5 halamanHubungan Hipertensi Dan Glycohemoglobin (Hba1c) Dengan Kejadian Retinopati Diabetik Pada Penderita Diabetes Melitus Di Rsud Margono Soekarjo PurwokertoNur HaniBelum ada peringkat
- Acute Diarrhea LaDokumen38 halamanAcute Diarrhea LaBane LtpBelum ada peringkat
- Troublesome Throat Awareness (tTA) As A Contemporary Alternative To 'Globus Pharyngeus (DOODY 2017)Dokumen3 halamanTroublesome Throat Awareness (tTA) As A Contemporary Alternative To 'Globus Pharyngeus (DOODY 2017)DANDYBelum ada peringkat
- Psychological Problems Associated With Thalassemia in Diyala Province, Iraq - OdtDokumen6 halamanPsychological Problems Associated With Thalassemia in Diyala Province, Iraq - OdtThe Swedish Journal of Scientific Research (SJSR) ISSN: 2001-9211Belum ada peringkat
- Syphilis SeroDokumen52 halamanSyphilis Seromarie judimor gomezBelum ada peringkat
- Acute Adverse Effects of TransfusionDokumen64 halamanAcute Adverse Effects of TransfusionArifudin Cipto HusodoBelum ada peringkat
- Manual Handling Case Studies Part 1 - Attempt Review PDFDokumen30 halamanManual Handling Case Studies Part 1 - Attempt Review PDFMODI KRUNAL100% (2)
- 2009 Nec Hiv Dec Aidsreg2009Dokumen3 halaman2009 Nec Hiv Dec Aidsreg2009Jing CruzBelum ada peringkat
- 139-Article Text-416-1-10-20180204Dokumen3 halaman139-Article Text-416-1-10-20180204Kriti KumariBelum ada peringkat
- cIMPACT-NOW Update 2 Diagnostic Clarifications For Diffuse Midline Glioma, H3 K27M-mutant and Diffuse Astrocytomaanaplastic Astrocytoma, IDH-mutantDokumen4 halamancIMPACT-NOW Update 2 Diagnostic Clarifications For Diffuse Midline Glioma, H3 K27M-mutant and Diffuse Astrocytomaanaplastic Astrocytoma, IDH-mutantDTBelum ada peringkat
- 19.sinonasal TumorsDokumen246 halaman19.sinonasal Tumorsfabian hernandez medinaBelum ada peringkat
- KNGF Guideline For Physical Therapy in Patients With ParkinsDokumen89 halamanKNGF Guideline For Physical Therapy in Patients With ParkinsSrđan ŠarenacBelum ada peringkat
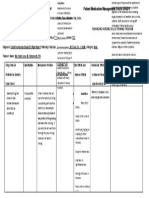
- Patient 1 Drug Study 1Dokumen1 halamanPatient 1 Drug Study 1Memcom SolutionBelum ada peringkat
- Eating DisordersDokumen15 halamanEating DisordersJana Marie CorpuzBelum ada peringkat
- Virtual Watcher's Class: Covid-19 N-E-W-S: Everything You Need To "Navigate" Through The New NormalDokumen27 halamanVirtual Watcher's Class: Covid-19 N-E-W-S: Everything You Need To "Navigate" Through The New NormalValerie FischerBelum ada peringkat
- Power Point Treatment of Functional Dyspepsia With SertralineDokumen26 halamanPower Point Treatment of Functional Dyspepsia With SertralineRadias ZasraBelum ada peringkat
- Isolated Glomerular Diseases Associated With Recurrent Gross HematuriaDokumen17 halamanIsolated Glomerular Diseases Associated With Recurrent Gross HematuriaMay PingolBelum ada peringkat
- Med Term 3 (1) - 231209 - 003105Dokumen30 halamanMed Term 3 (1) - 231209 - 003105Anushka KarthikeyanBelum ada peringkat
- Ascvd Risk Score 062719 KroDokumen1 halamanAscvd Risk Score 062719 KroQuang TranBelum ada peringkat
- This Is Known As Student DiversityDokumen3 halamanThis Is Known As Student DiversityAngela Marie Hilario PacursaBelum ada peringkat
- Blood and Tissue NematodesDokumen60 halamanBlood and Tissue NematodesDanielle Pecson100% (1)
- Journal Homepage: - : IntroductionDokumen5 halamanJournal Homepage: - : IntroductionIJAR JOURNALBelum ada peringkat
- Peptic UlcerDokumen4 halamanPeptic UlcerEris Abdul AzizBelum ada peringkat
- Environmental Science and Engineering: Case Study #7: Covid-19 Name: Manglo, John Andrae BDokumen1 halamanEnvironmental Science and Engineering: Case Study #7: Covid-19 Name: Manglo, John Andrae BJohn Andrae MangloBelum ada peringkat
- ReflectionDokumen4 halamanReflectionelizaviraniBelum ada peringkat
- PSYCH - 1st Sem Finals FeedbackDokumen2 halamanPSYCH - 1st Sem Finals FeedbackEricBelum ada peringkat
- Lupus: PrintDokumen24 halamanLupus: Printmelodia gandezaBelum ada peringkat
- WSDDokumen13 halamanWSDhinatakunhinata75Belum ada peringkat
- Cardiopulmonary Arrest Simulation LabDokumen3 halamanCardiopulmonary Arrest Simulation LabJessica Mason100% (2)
- Management of Medically Compromised PatientsDokumen70 halamanManagement of Medically Compromised PatientsPriyanka WadhawanBelum ada peringkat
- Abbott 26090 CAG Brochure r2 ZincDokumen24 halamanAbbott 26090 CAG Brochure r2 ZinctheresmariajBelum ada peringkat
- Breaking the Habit of Being YourselfDari EverandBreaking the Habit of Being YourselfPenilaian: 4.5 dari 5 bintang4.5/5 (1458)
- Sleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningDari EverandSleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningPenilaian: 4 dari 5 bintang4/5 (3)
- Summary of The 4-Hour Body: An Uncommon Guide to Rapid Fat-Loss, Incredible Sex, and Becoming Superhuman by Timothy FerrissDari EverandSummary of The 4-Hour Body: An Uncommon Guide to Rapid Fat-Loss, Incredible Sex, and Becoming Superhuman by Timothy FerrissPenilaian: 4.5 dari 5 bintang4.5/5 (81)
- Peaceful Sleep Hypnosis: Meditate & RelaxDari EverandPeaceful Sleep Hypnosis: Meditate & RelaxPenilaian: 4.5 dari 5 bintang4.5/5 (142)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisDari EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisPenilaian: 4 dari 5 bintang4/5 (1)
- The Comfort of Crows: A Backyard YearDari EverandThe Comfort of Crows: A Backyard YearPenilaian: 4.5 dari 5 bintang4.5/5 (23)
- Forever Strong: A New, Science-Based Strategy for Aging WellDari EverandForever Strong: A New, Science-Based Strategy for Aging WellBelum ada peringkat
- The Happiest Baby on the Block: The New Way to Calm Crying and Help Your Newborn Baby Sleep LongerDari EverandThe Happiest Baby on the Block: The New Way to Calm Crying and Help Your Newborn Baby Sleep LongerPenilaian: 4.5 dari 5 bintang4.5/5 (58)
- How to Talk to Anyone: Learn the Secrets of Good Communication and the Little Tricks for Big Success in RelationshipDari EverandHow to Talk to Anyone: Learn the Secrets of Good Communication and the Little Tricks for Big Success in RelationshipPenilaian: 4.5 dari 5 bintang4.5/5 (1135)
- Gut Health Hacks: 200 Ways to Balance Your Gut Microbiome and Improve Your Health!Dari EverandGut Health Hacks: 200 Ways to Balance Your Gut Microbiome and Improve Your Health!Penilaian: 4.5 dari 5 bintang4.5/5 (20)
- Love Yourself, Heal Your Life Workbook (Insight Guide)Dari EverandLove Yourself, Heal Your Life Workbook (Insight Guide)Penilaian: 5 dari 5 bintang5/5 (40)
- Deep Sleep Hypnosis: Guided Meditation For Sleep & HealingDari EverandDeep Sleep Hypnosis: Guided Meditation For Sleep & HealingPenilaian: 4.5 dari 5 bintang4.5/5 (103)
- 369: Manifesting Through 369 and the Law of Attraction - METHODS, TECHNIQUES AND EXERCISESDari Everand369: Manifesting Through 369 and the Law of Attraction - METHODS, TECHNIQUES AND EXERCISESPenilaian: 5 dari 5 bintang5/5 (50)
- Really Very Crunchy: A Beginner's Guide to Removing Toxins from Your Life without Adding Them to Your PersonalityDari EverandReally Very Crunchy: A Beginner's Guide to Removing Toxins from Your Life without Adding Them to Your PersonalityPenilaian: 5 dari 5 bintang5/5 (28)
- Deep Sleep Meditation: Fall Asleep Instantly with Powerful Guided Meditations, Hypnosis, and Affirmations. Overcome Anxiety, Depression, Insomnia, Stress, and Relax Your Mind!Dari EverandDeep Sleep Meditation: Fall Asleep Instantly with Powerful Guided Meditations, Hypnosis, and Affirmations. Overcome Anxiety, Depression, Insomnia, Stress, and Relax Your Mind!Penilaian: 4.5 dari 5 bintang4.5/5 (10)
- Bedtime Stories for Adults: Tales to Soothe the Tired SoulsDari EverandBedtime Stories for Adults: Tales to Soothe the Tired SoulsPenilaian: 4 dari 5 bintang4/5 (3)
- Aging Backwards: Reverse the Aging Process and Look 10 Years Younger in 30 Minutes a DayDari EverandAging Backwards: Reverse the Aging Process and Look 10 Years Younger in 30 Minutes a DayBelum ada peringkat
- Chair Yoga: Sit, Stretch, and Strengthen Your Way to a Happier, Healthier YouDari EverandChair Yoga: Sit, Stretch, and Strengthen Your Way to a Happier, Healthier YouPenilaian: 3.5 dari 5 bintang3.5/5 (5)
- The Beck Diet Solution Weight Loss Workbook: The 6-Week Plan to Train Your Brain to Think Like a Thin PersonDari EverandThe Beck Diet Solution Weight Loss Workbook: The 6-Week Plan to Train Your Brain to Think Like a Thin PersonPenilaian: 3.5 dari 5 bintang3.5/5 (33)
- The Well-Lived Life: A 102-Year-Old Doctor's Six Secrets to Health and Happiness at Every AgeDari EverandThe Well-Lived Life: A 102-Year-Old Doctor's Six Secrets to Health and Happiness at Every AgePenilaian: 4.5 dari 5 bintang4.5/5 (30)
- Instant Loss On a Budget: Super-Affordable Recipes for the Health-Conscious CookDari EverandInstant Loss On a Budget: Super-Affordable Recipes for the Health-Conscious CookPenilaian: 3.5 dari 5 bintang3.5/5 (2)
- The Longevity Book: The Science of Aging, the Biology of Strength, and the Privilege of TimeDari EverandThe Longevity Book: The Science of Aging, the Biology of Strength, and the Privilege of TimePenilaian: 3.5 dari 5 bintang3.5/5 (13)
- Deep Sleep Hypnosis: Fall Asleep Instantly And Sleep WellDari EverandDeep Sleep Hypnosis: Fall Asleep Instantly And Sleep WellPenilaian: 5 dari 5 bintang5/5 (8)
- Metabolism Revolution: Lose 14 Pounds in 14 Days and Keep It Off for LifeDari EverandMetabolism Revolution: Lose 14 Pounds in 14 Days and Keep It Off for LifeBelum ada peringkat