Anda mungkin juga menyukai
- Blumgart's Surgery of The Liver, Biliary Tract, and Pancreas 6ed 2017 2vols 2401pag PDFDokumen2.401 halamanBlumgart's Surgery of The Liver, Biliary Tract, and Pancreas 6ed 2017 2vols 2401pag PDFLucia Maria De Castro Mendes92% (26)
- Nursing Education: Leading the TransformationDokumen31 halamanNursing Education: Leading the TransformationDip Ayan M100% (1)
- Acute Renal FailureDokumen33 halamanAcute Renal FailureAqsa Akbar AliBelum ada peringkat
- Organ Donation A Persuasive Speech by Mikayla NogueiraDokumen3 halamanOrgan Donation A Persuasive Speech by Mikayla Nogueiraapi-475986633Belum ada peringkat
- MT Carmel 50 Anniversary WebDokumen104 halamanMT Carmel 50 Anniversary WebMartin GohBelum ada peringkat
- Management Question PaperDokumen23 halamanManagement Question Papersarajacob2000.adonaiBelum ada peringkat
- ChemotherapyDokumen35 halamanChemotherapynikhl saulBelum ada peringkat
- Drugs Used in CPR - Lesson PlanDokumen12 halamanDrugs Used in CPR - Lesson Planmonika makwana100% (2)
- Prepared By: Athulya G Ii Year MSC Nursing Upasana College of Nursing KollamDokumen25 halamanPrepared By: Athulya G Ii Year MSC Nursing Upasana College of Nursing KollamGayathri RBelum ada peringkat
- Hypertension Prepost Test - Answer KeyDokumen3 halamanHypertension Prepost Test - Answer Keyapi-247079964100% (1)
- Post-Debridement Nursing Care PlanDokumen2 halamanPost-Debridement Nursing Care PlanAbdelmar SusulanBelum ada peringkat
- Assessment of Renal and Urinary Tract FunctionDokumen19 halamanAssessment of Renal and Urinary Tract FunctionokaciaBelum ada peringkat
- Terminologies Used in Nursing Education 1Dokumen11 halamanTerminologies Used in Nursing Education 1ramita sahBelum ada peringkat
- Stages of Labor BrochureDokumen2 halamanStages of Labor Brochureapi-273000494100% (1)
- Evaluation FormatDokumen4 halamanEvaluation FormatKinjal VasavaBelum ada peringkat
- Peptic Ulcer Disease: Causes, Symptoms and TreatmentDokumen60 halamanPeptic Ulcer Disease: Causes, Symptoms and TreatmentNehimyaBelum ada peringkat
- Cardiac Diet HandoutDokumen2 halamanCardiac Diet Handoutapi-537434972Belum ada peringkat
- GERIATRIC CONSIDERATIONS IN NURSINGDokumen70 halamanGERIATRIC CONSIDERATIONS IN NURSINGsanthiyasandy100% (1)
- Pooja FinalDokumen35 halamanPooja FinalSagar ChiplunkarBelum ada peringkat
- Compartment Syndrome Diagnosis and TreatmentDokumen3 halamanCompartment Syndrome Diagnosis and TreatmentTantyo Adi P100% (2)
- Ethics in Nursing ResearchDokumen17 halamanEthics in Nursing Researchنادر القحطانيBelum ada peringkat
- Epidemilogy Measurment MethodsDokumen100 halamanEpidemilogy Measurment MethodsKailash NagarBelum ada peringkat
- NVD With EpisiotomyDokumen4 halamanNVD With EpisiotomySimran SimzBelum ada peringkat
- Nursing Responsibilities of Hematinic DrugsDokumen1 halamanNursing Responsibilities of Hematinic DrugsStudent Nurse0% (1)
- Drugs: Oxytocin: Presented By: Ms. Ankita Lal Lecturer Department of Obstetrics & GynecologyDokumen8 halamanDrugs: Oxytocin: Presented By: Ms. Ankita Lal Lecturer Department of Obstetrics & GynecologyPrincess LizaBelum ada peringkat
- Applying Orem's Theory to Improve NutritionDokumen12 halamanApplying Orem's Theory to Improve NutritionAnnapurna DangetiBelum ada peringkat
- Research ProposalDokumen22 halamanResearch ProposalKapil LakhwaraBelum ada peringkat
- Kidney Stones: Causes, Symptoms and TreatmentDokumen26 halamanKidney Stones: Causes, Symptoms and TreatmentPatrascu CristiBelum ada peringkat
- D.S.S Aiims Prepration Test Series - 9Dokumen28 halamanD.S.S Aiims Prepration Test Series - 9Dr-Sanjay SinghaniaBelum ada peringkat
- Nursing Care Plan On: Ca OvaryDokumen13 halamanNursing Care Plan On: Ca Ovaryvaishali TayadeBelum ada peringkat
- HypomagnesemiaDokumen7 halamanHypomagnesemiaNader SmadiBelum ada peringkat
- Nursing Council of KenyaDokumen6 halamanNursing Council of Kenyageorgeloto12100% (1)
- Puerperium Q ADokumen2 halamanPuerperium Q AMae Rose Charlene MendozaBelum ada peringkat
- Live Preterm Baby Delivered NSDDokumen13 halamanLive Preterm Baby Delivered NSDKristine Anne SorianoBelum ada peringkat
- ICDS Scheme ExplainedDokumen59 halamanICDS Scheme ExplainedRamniwasMahoreBelum ada peringkat
- Acute Renal FailureDokumen17 halamanAcute Renal FailureDina Rasmita100% (1)
- DEFINITION: Abortion Is The Expulsion or Extraction From Its MotherDokumen10 halamanDEFINITION: Abortion Is The Expulsion or Extraction From Its MothermOHAN.SBelum ada peringkat
- Developing Theoretical and Conceptual Frameworks and Operational Definition of TermsDokumen44 halamanDeveloping Theoretical and Conceptual Frameworks and Operational Definition of TermsHTCCS BatoCamSurBelum ada peringkat
- Blunt Force Trauma-FinalDokumen73 halamanBlunt Force Trauma-FinalHera Khaeyratul HisannBelum ada peringkat
- Mental Health Nursing Exam QuestionsDokumen17 halamanMental Health Nursing Exam QuestionsSubiVictorBelum ada peringkat
- M.SC Nursing Syllabus Revised 2018 - 19-23082019-1Dokumen344 halamanM.SC Nursing Syllabus Revised 2018 - 19-23082019-1Divya ToppoBelum ada peringkat
- Lecture 6 Pain Management in Children by Pharmacological and NonDokumen25 halamanLecture 6 Pain Management in Children by Pharmacological and NonRubinaBelum ada peringkat
- Knowledge Regarding Skin Banking Among Student NursesDokumen5 halamanKnowledge Regarding Skin Banking Among Student NursesAnonymous izrFWiQBelum ada peringkat
- Care of Patient With AnorexiaDokumen14 halamanCare of Patient With Anorexiavaishali TMU studentBelum ada peringkat
- ETHICO OutlineDokumen5 halamanETHICO Outline'emotera' Gudbai DotaBelum ada peringkat
- EpispadiasisDokumen12 halamanEpispadiasisvishnuBelum ada peringkat
- CellulitisDokumen15 halamanCellulitisSujatha J JayabalBelum ada peringkat
- Urine Collection: - Clinical Instructor (Sign Over Printed Name)Dokumen2 halamanUrine Collection: - Clinical Instructor (Sign Over Printed Name)hey aadarshaBelum ada peringkat
- Abruption Placenta Definition Causes Symptoms ManagementDokumen30 halamanAbruption Placenta Definition Causes Symptoms ManagementArchana MaharjanBelum ada peringkat
- Essential Components of Palliative CareDokumen13 halamanEssential Components of Palliative Careleian28100% (1)
- Food HygieneDokumen31 halamanFood Hygienehemihema100% (1)
- Anticougulation in PregnancyDokumen21 halamanAnticougulation in PregnancyLubna AliBelum ada peringkat
- OSCE Subcutaneous Injection SkillsDokumen2 halamanOSCE Subcutaneous Injection SkillsvishnuBelum ada peringkat
- ChemotherapyDokumen11 halamanChemotherapyRekha G.Belum ada peringkat
- CET Principles of Education & Teaching Learning Process (39Dokumen40 halamanCET Principles of Education & Teaching Learning Process (39Ellen AngelBelum ada peringkat
- Colostomy CareDokumen2 halamanColostomy CareMel RodolfoBelum ada peringkat
- History of Icommunity Health NursingDokumen37 halamanHistory of Icommunity Health NursingNeenu RajputBelum ada peringkat
- PCNL Nursing Care Plan 2Dokumen11 halamanPCNL Nursing Care Plan 2ISICLE GTBelum ada peringkat
- Community As Client PDFDokumen2 halamanCommunity As Client PDFNathan0% (1)
- 1 - Nursing - Status - and - ImageDokumen66 halaman1 - Nursing - Status - and - ImagePriya bhattiBelum ada peringkat
- Emergency DrugsDokumen5 halamanEmergency DrugsCatherine Martinez AvilaBelum ada peringkat
- Hirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDari EverandHirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsBelum ada peringkat
- Ebstein Anomaly, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDari EverandEbstein Anomaly, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsBelum ada peringkat
- Skin Diseases Disorders ConditionsDokumen104 halamanSkin Diseases Disorders ConditionsJerilee SoCute WattsBelum ada peringkat
- Reproduction and DevelopmentDokumen53 halamanReproduction and DevelopmentJerilee SoCute WattsBelum ada peringkat
- PDFDokumen64 halamanPDFJerilee SoCute WattsBelum ada peringkat
- SkinDokumen43 halamanSkinFhen Farrel100% (1)
- Respiratory System 2Dokumen39 halamanRespiratory System 2Jerilee SoCute WattsBelum ada peringkat
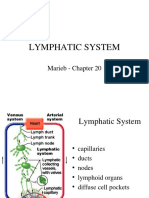
- The Lymphatic SystemDokumen50 halamanThe Lymphatic SystemJerilee SoCute Watts100% (1)
- The Circulatory System-: TransportDokumen13 halamanThe Circulatory System-: TransportJerilee SoCute WattsBelum ada peringkat
- Digestive SystemDokumen48 halamanDigestive SystemJerilee SoCute WattsBelum ada peringkat
- CV SYSTEM ANATOMYDokumen42 halamanCV SYSTEM ANATOMYJerilee SoCute WattsBelum ada peringkat
- Reproductive SystemDokumen80 halamanReproductive SystemJerilee SoCute WattsBelum ada peringkat
- Digestive System: Stomach and Small Intestine FunctionsDokumen56 halamanDigestive System: Stomach and Small Intestine FunctionsJerilee SoCute WattsBelum ada peringkat
- Lecture 21 - Respiratory SystemDokumen59 halamanLecture 21 - Respiratory SystemSkyBirdBelum ada peringkat
- Urinary SystemDokumen105 halamanUrinary SystemJerilee SoCute WattsBelum ada peringkat
- The Digestive System Part 1Dokumen28 halamanThe Digestive System Part 1Jerilee SoCute WattsBelum ada peringkat
- The Conducting System of The HeartDokumen37 halamanThe Conducting System of The HeartJerilee SoCute WattsBelum ada peringkat
- Respiratory System Anatomy and Functions EX36Dokumen57 halamanRespiratory System Anatomy and Functions EX36royanirudh99Belum ada peringkat
- Pulmonary and Systemic CircuitsDokumen38 halamanPulmonary and Systemic CircuitsJerilee SoCute WattsBelum ada peringkat
- The Digestive System EssayDokumen3 halamanThe Digestive System EssayJerilee SoCute Watts0% (1)
- Lymphatic System: Marieb Chapter 20Dokumen22 halamanLymphatic System: Marieb Chapter 20Jerilee SoCute WattsBelum ada peringkat
- Brain Respiratory Centers & Control MechanismsDokumen36 halamanBrain Respiratory Centers & Control MechanismsJerilee SoCute WattsBelum ada peringkat
- Respiratory System 1Dokumen29 halamanRespiratory System 1Jerilee SoCute WattsBelum ada peringkat
- Review Questions - Heart Anatomy & PhysiologyDokumen1 halamanReview Questions - Heart Anatomy & PhysiologyJerilee SoCute WattsBelum ada peringkat
- Reproductive System DisordersDokumen62 halamanReproductive System DisordersJerilee SoCute Watts100% (2)
- Human ReproductionDokumen42 halamanHuman ReproductionAliDarimiKRBelum ada peringkat
- Reproduction NotesDokumen20 halamanReproduction NotesMario BaemamentengBelum ada peringkat
- Reproduction Summary NotesDokumen16 halamanReproduction Summary NotesJerilee SoCute WattsBelum ada peringkat
- Lecture 1 Cardiovascular SystemDokumen70 halamanLecture 1 Cardiovascular SystemJerilee SoCute WattsBelum ada peringkat
- Platelets and HemostasisDokumen19 halamanPlatelets and HemostasisJerilee SoCute WattsBelum ada peringkat
- Unit 6 OsmolarityDokumen59 halamanUnit 6 Osmolaritykrystal1994Belum ada peringkat
- Past Papers Section2Dokumen13 halamanPast Papers Section2Jerilee SoCute Watts50% (2)
- Advances in Malignant Melanoma - Clinical and Research PerspectivesDokumen264 halamanAdvances in Malignant Melanoma - Clinical and Research PerspectivesInternational Medical PublisherBelum ada peringkat
- Interpol Report 2021Dokumen38 halamanInterpol Report 2021Local12wkrcBelum ada peringkat
- Winona Health - Healthy Connections Spring 2007Dokumen16 halamanWinona Health - Healthy Connections Spring 2007winonahealthBelum ada peringkat
- Baylor ST Luke's Hospital - DR Deborah MeyersDokumen3 halamanBaylor ST Luke's Hospital - DR Deborah MeyersCBS This MorningBelum ada peringkat
- Should We Allow the Sale of Human OrgansDokumen3 halamanShould We Allow the Sale of Human OrgansMegat MahathirBelum ada peringkat
- Evaluacion Pulmonar PreoperatoriaDokumen15 halamanEvaluacion Pulmonar Preoperatorialuis castillejosBelum ada peringkat
- Sample Persuasive SpeechDokumen2 halamanSample Persuasive SpeechViven DranBelum ada peringkat
- Aplastic Anemia Symptoms, Causes, TreatmentsDokumen19 halamanAplastic Anemia Symptoms, Causes, TreatmentsNadia Puspita DewiBelum ada peringkat
- McARDLE Jack - 150 Stories For Preachers and TeachersDokumen49 halamanMcARDLE Jack - 150 Stories For Preachers and TeachersbabiboibanBelum ada peringkat
- Kidney Transplantation: A Guide to Renal Transplantation Procedures & Living Donor OptionsDokumen5 halamanKidney Transplantation: A Guide to Renal Transplantation Procedures & Living Donor OptionsDeadly ChillerBelum ada peringkat
- Four key ethical principles in healthcareDokumen27 halamanFour key ethical principles in healthcareFREDDIE BISQUERA IIBelum ada peringkat
- Ethics and Genetic EngineeringDokumen37 halamanEthics and Genetic EngineeringbhaskarbanerjiBelum ada peringkat
- Organ Trafficking in IndiaDokumen4 halamanOrgan Trafficking in IndiaKandlagunta Gayathri PraharshithaBelum ada peringkat
- AMA Code of Ethics For Behavior ScienceDokumen63 halamanAMA Code of Ethics For Behavior Scienceمحمد ضياءBelum ada peringkat
- Mock Paper 2Dokumen32 halamanMock Paper 2Bala JishnuBelum ada peringkat
- Case#4 - Dioquino, Myka EllaDokumen2 halamanCase#4 - Dioquino, Myka EllaMyka Ella DioquinoBelum ada peringkat
- Kidney Trafficking in NepalDokumen124 halamanKidney Trafficking in NepalBistea Iuliana ElenaBelum ada peringkat
- Living Donor Transplantation BrochureDokumen13 halamanLiving Donor Transplantation BrochureShani KushwahaBelum ada peringkat
- JAP130 Slides 6Dokumen5 halamanJAP130 Slides 6smpn1 PabuaranBelum ada peringkat
- ESOT 2015 Advanced ProgramDokumen33 halamanESOT 2015 Advanced ProgramFrancescoBelum ada peringkat
- R.A. 7170 Organ DonationDokumen5 halamanR.A. 7170 Organ DonationAir Dela CruzBelum ada peringkat
- Annual Report 2009 - 2010Dokumen56 halamanAnnual Report 2009 - 2010St George's Healthcare NHS TrustBelum ada peringkat
- HLA Sensitisation - Can It Be PreventedDokumen11 halamanHLA Sensitisation - Can It Be PreventedPatriciaBelum ada peringkat
- GENERAL EDUCATION Test Material 198 ItemsDokumen13 halamanGENERAL EDUCATION Test Material 198 ItemsBM Ayunnie VlogBelum ada peringkat
- Literature ReviewDokumen11 halamanLiterature Reviewapi-691127747Belum ada peringkat
- Online Organ Donation Using BlockchainDokumen7 halamanOnline Organ Donation Using BlockchainIJRASETPublicationsBelum ada peringkat
- CRISTIAN COLCERIU ELITE CLUJENE Prof - Univ.Dr. MIHAI LUCANDokumen15 halamanCRISTIAN COLCERIU ELITE CLUJENE Prof - Univ.Dr. MIHAI LUCANcristian colceriu100% (2)